Department of Radiation Physics, The University of Texas MD Anderson Cancer Center, Houston, TX 77030, United States of America. Author to whom any correspondence should be addressed.
Phys Med Biol. 2017 Dec 19;63(1):015013. doi: 10.1088/1361-6560/aa9a2e.
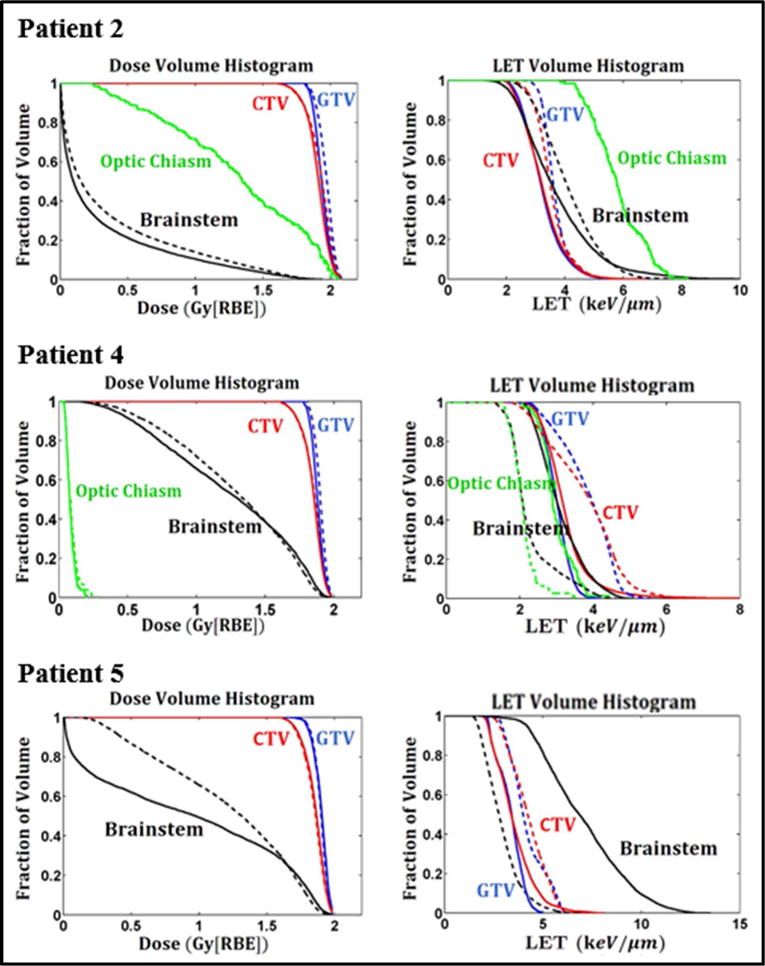
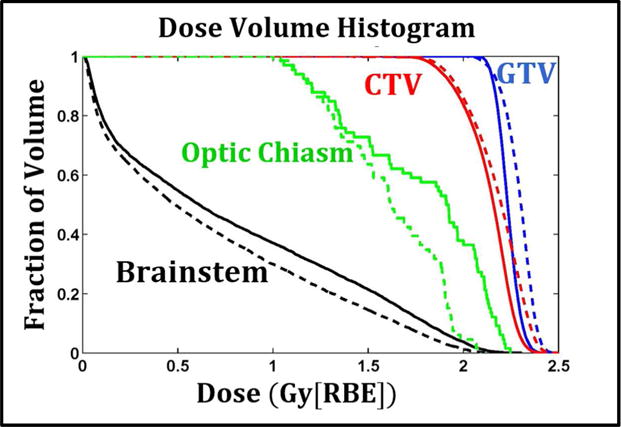
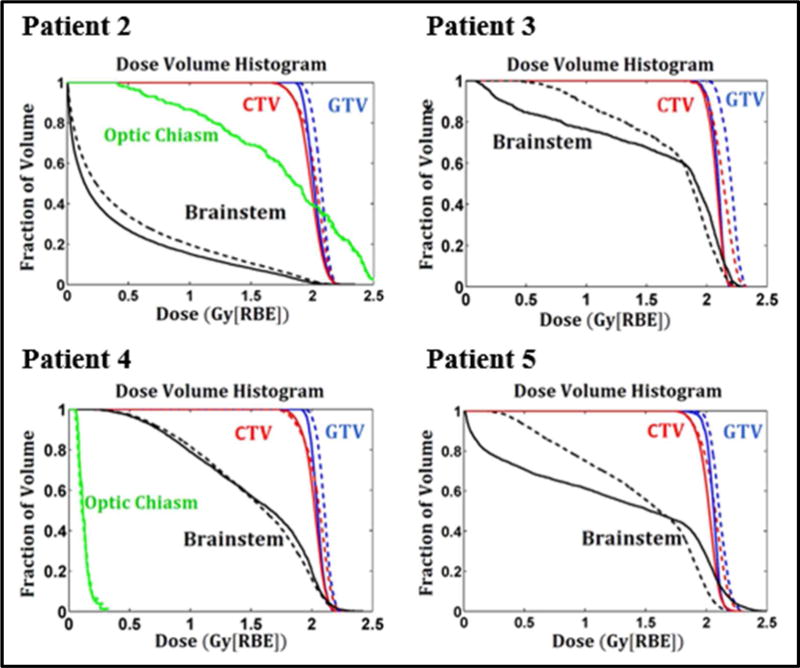
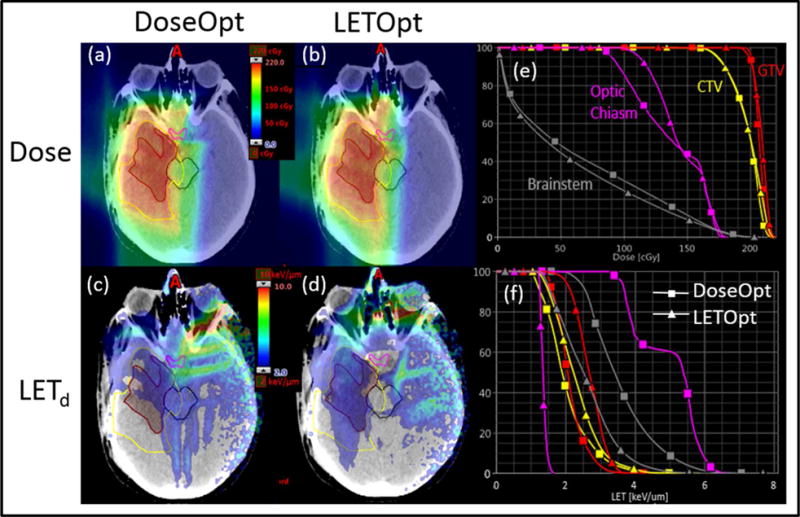
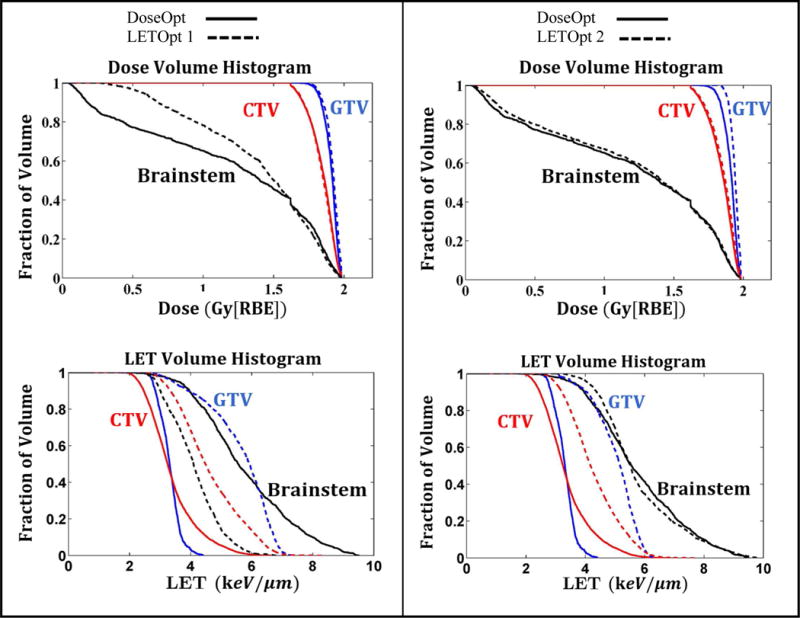
The purpose of this study was to investigate the feasibility of incorporating linear energy transfer (LET) into the optimization of intensity modulated proton therapy (IMPT) plans. Because increased LET correlates with increased biological effectiveness of protons, high LETs in target volumes and low LETs in critical structures and normal tissues are preferred in an IMPT plan. However, if not explicitly incorporated into the optimization criteria, different IMPT plans may yield similar physical dose distributions but greatly different LET, specifically dose-averaged LET, distributions. Conventionally, the IMPT optimization criteria (or cost function) only includes dose-based objectives in which the relative biological effectiveness (RBE) is assumed to have a constant value of 1.1. In this study, we added LET-based objectives for maximizing LET in target volumes and minimizing LET in critical structures and normal tissues. Due to the fractional programming nature of the resulting model, we used a variable reformulation approach so that the optimization process is computationally equivalent to conventional IMPT optimization. In this study, five brain tumor patients who had been treated with proton therapy at our institution were selected. Two plans were created for each patient based on the proposed LET-incorporated optimization (LETOpt) and the conventional dose-based optimization (DoseOpt). The optimized plans were compared in terms of both dose (assuming a constant RBE of 1.1 as adopted in clinical practice) and LET. Both optimization approaches were able to generate comparable dose distributions. The LET-incorporated optimization achieved not only pronounced reduction of LET values in critical organs, such as brainstem and optic chiasm, but also increased LET in target volumes, compared to the conventional dose-based optimization. However, on occasion, there was a need to tradeoff the acceptability of dose and LET distributions. Our conclusion is that the inclusion of LET-dependent criteria in the IMPT optimization could lead to similar dose distributions as the conventional optimization but superior LET distributions in target volumes and normal tissues. This may have substantial advantages in improving tumor control and reducing normal tissue toxicities.
本研究旨在探讨将线性能量传递(LET)纳入调强质子治疗(IMPT)计划优化的可行性。由于 LET 增加与质子生物学效应增加相关,因此在 IMPT 计划中,靶区中应采用高 LET,而在危及器官和正常组织中应采用低 LET。然而,如果没有明确纳入优化标准,不同的 IMPT 计划可能会产生相似的物理剂量分布,但 LET,特别是剂量平均 LET 分布会有很大差异。传统上,IMPT 优化标准(或成本函数)仅包括基于剂量的目标,其中相对生物学效应(RBE)被假定为恒定值 1.1。在本研究中,我们添加了基于 LET 的目标,以最大化靶区中的 LET,并最小化危及器官和正常组织中的 LET。由于所得到的模型具有分数规划性质,我们使用了变量重述方法,以使优化过程在计算上等效于传统的 IMPT 优化。在本研究中,选择了在我们机构接受质子治疗的五名脑肿瘤患者。为每位患者基于提出的包含 LET 的优化(LETOpt)和传统的基于剂量的优化(DoseOpt)创建了两个计划。基于剂量(采用临床实践中采用的恒定 RBE 值 1.1)和 LET 比较了优化计划。两种优化方法都能够生成可比的剂量分布。与传统的基于剂量的优化相比,包含 LET 的优化不仅实现了危及器官(如脑干和视交叉)中的 LET 值显著降低,而且还提高了靶区中的 LET。然而,有时需要权衡剂量和 LET 分布的可接受性。我们的结论是,在 IMPT 优化中包含 LET 相关标准可能会导致与传统优化相似的剂量分布,但在靶区和正常组织中具有更好的 LET 分布。这可能在提高肿瘤控制和降低正常组织毒性方面具有重要优势。