Weum Abrahamsen Ingerid, Grønvold Bjørn Christer, Inderberg Else Marit, Mensali Nadia, Mattsson Jonas, Gedde-Dahl Tobias
Department of Hematology, Oslo University Hospital, Rikshospitalet, Oslo, Norway.
Department of Cellular Therapy, Department of Oncology, Oslo University Hospital, The Norwegian Radium Hospital, Oslo, Norway.
Case Reports Immunol. 2020 Feb 25;2020:9403123. doi: 10.1155/2020/9403123. eCollection 2020.
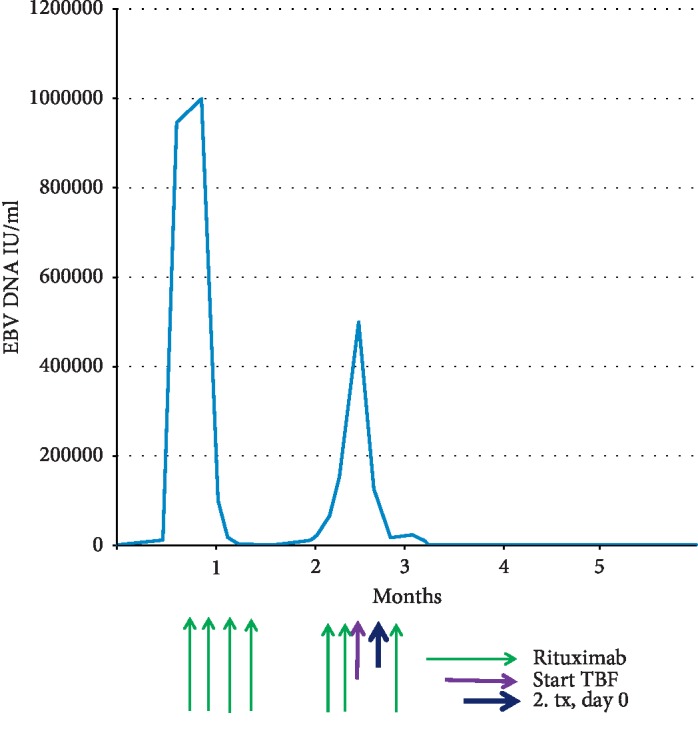
Epstein-Barr virus- (EBV-) induced posttransplantation lymphoproliferative disease (PTLD) is a life-threatening complication following allogeneic stem cell transplantation. The main risk factor is anti-thymocyte globulin (ATG). Patients who fail first-line treatment with rituximab have a poor prognosis. Though adoptive transfer of EBV-specific T cells is a potentially effective option, it is not readily available. In this case report, the patient developed PTLD following transplantation for aplastic anemia using ATG as part of the conditioning. He failed rituximab treatment and developed graft failure. We were aware that the stem cell donor had a recent EBV infection prior to transplantation, whereas the patient most likely was EBV negative before transplant. We describe our strategy to meet the patient's urgent need for EBV-specific T cells, as well as new hematopoietic stem cells. The same donor was used for a second transplant, using peripheral blood stem cells. The conditioning used was thiotepa/busulfan/fludarabin with a single dose of cyclophosphamide after transplant as graft-versus-host disease (GVHD) prophylaxis. The EBV DNA levels fell when conditioning was started, and have been undetectable since day +15 and remained so till 18 months after transplantation. The patient is doing well. This case reports successful use of cyclophosphamide after transplantation as GVHD prophylaxis, preserving virus-specific immunity.
爱泼斯坦-巴尔病毒(EBV)诱导的移植后淋巴细胞增生性疾病(PTLD)是异基因干细胞移植后一种危及生命的并发症。主要危险因素是抗胸腺细胞球蛋白(ATG)。一线使用利妥昔单抗治疗失败的患者预后较差。尽管过继转移EBV特异性T细胞是一种潜在有效的选择,但不易获得。在本病例报告中,患者因再生障碍性贫血接受移植,在预处理中使用了ATG,之后发生了PTLD。他的利妥昔单抗治疗失败,并出现了移植物功能衰竭。我们注意到干细胞供者在移植前近期有EBV感染,而患者在移植前很可能是EBV阴性。我们描述了满足患者对EBV特异性T细胞以及新的造血干细胞迫切需求的策略。使用同一供者进行第二次移植,采用外周血干细胞。预处理方案为噻替派/白消安/氟达拉滨,并在移植后使用单剂量环磷酰胺预防移植物抗宿主病(GVHD)。开始预处理时EBV DNA水平下降,自+15天起一直检测不到,直至移植后18个月仍保持如此。患者情况良好。本病例报告了移植后成功使用环磷酰胺预防GVHD,同时保留病毒特异性免疫。