Phanish Mysore K, Hull Richard P, Andrews Peter A, Popoola Joyce, Kingdon Edward J, MacPhee Iain A M
South West Thames Renal and Transplantation Unit, St Helier Hospital, Epsom and St Helier University Hospitals NHS trust, Carshalton, UK.
SW Thames Institute for Renal Research, St Helier Hospital, Carshalton, Surrey, SM5 1AA, UK.
BMC Nephrol. 2020 Mar 11;21(1):92. doi: 10.1186/s12882-020-01739-3.
The efficacy and safety of minimisation of immunosuppression including early steroid withdrawal in kidney transplant recipients treated with Basiliximab induction remains unclear.
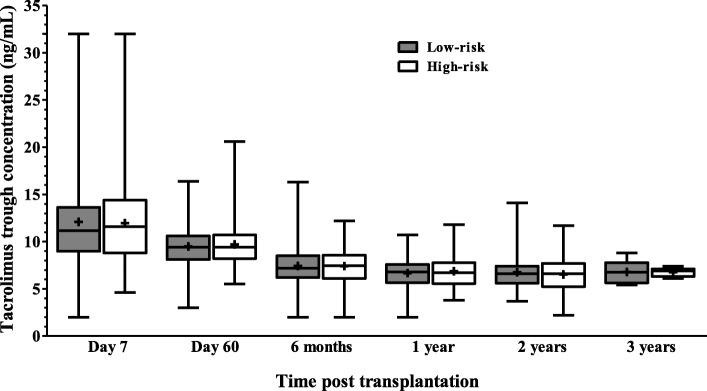
This retrospective cohort study reports the outcomes from 298 consecutive renal transplants performed since 1st July 2010-June 2013 treated with Basiliximab induction and early steroid withdrawal in low immunological risk patients using a simple immunological risk stratification and 3-month protocol biopsy to optimise therapy. The cohort comprised 225 low-risk patients (first transplant or HLA antibody calculated reaction frequency (CRF ≤50% with no donor specific HLA antibodies) who underwent basiliximab induction, steroid withdrawal on day 7 and maintenance with tacrolimus and mycophenolate mofetil (MMF), and 73 high-risk patients who received tacrolimus, MMF and prednisolone for the first 3 months followed by long term maintenance immunosuppression with tacrolimus and prednisolone. High-risk patients not undergoing 3-month protocol biopsy were continued on triple immunosuppression.
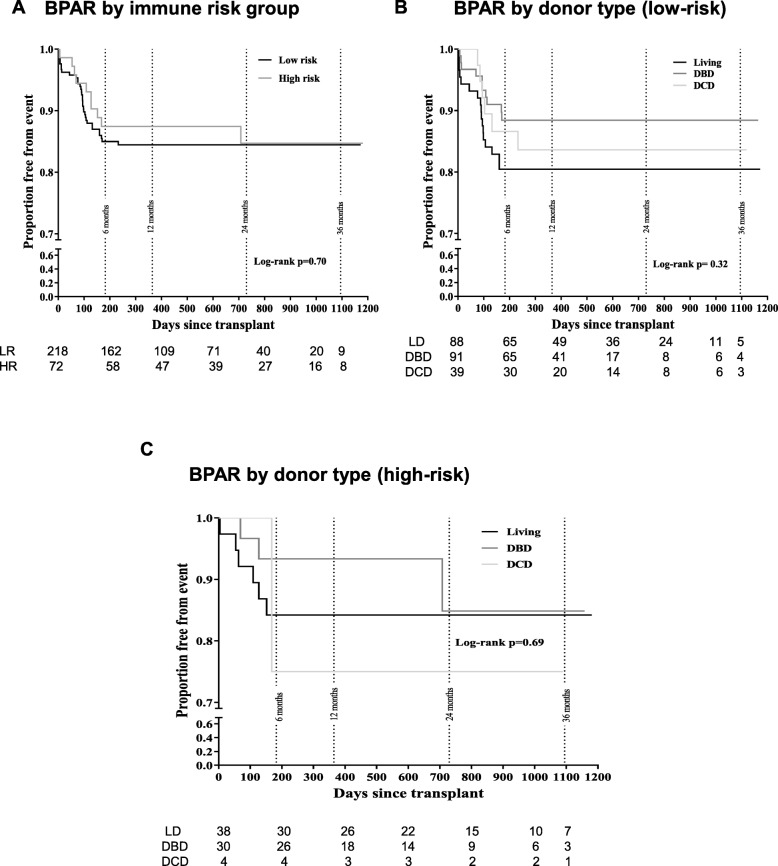
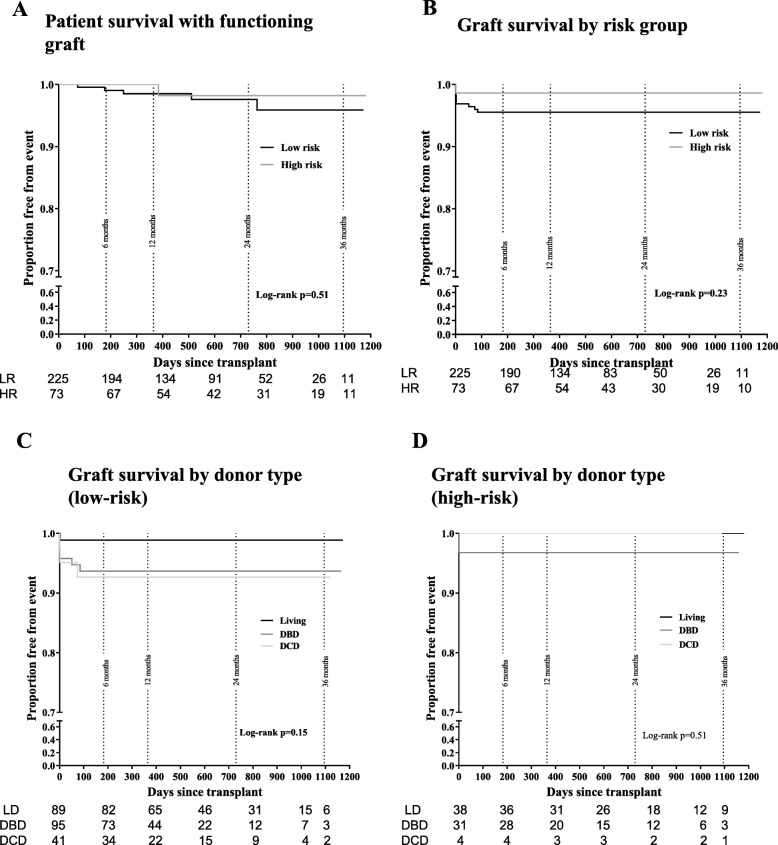
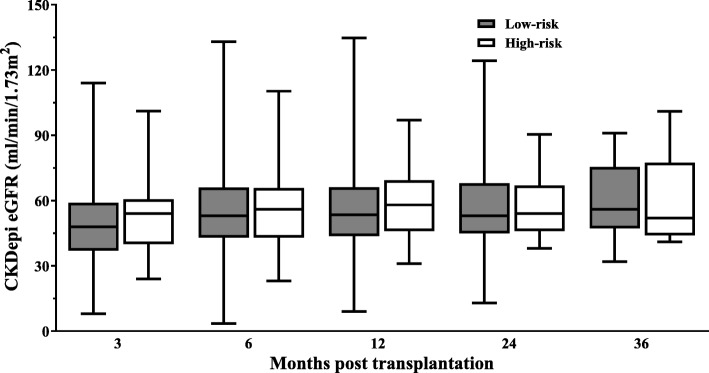
Steroid withdrawal could be safely achieved in low immunological risk recipients with IL2 receptor antibody induction. The incidence of biopsy-proven acute rejection was 15.1% in the low-risk and 13.9% in the high-risk group (including sub-clinical rejection detected at protocol biopsy). One- year graft survival was 93.3% and patient survival 98.5% in the low-risk group, and 97.3 and 100% respectively in the high-risk group. Graft function was similar in each group at 1 year (mean eGFR 61.2 ± 23.4 mL/min low-risk and 64.6 ± 19.2 mL/min high-risk).
Immunosuppression regimen comprising basiliximab induction, tacrolimus, MMF and prednisolone with early steroid withdrawal in low risk patients and MMF withdrawal in high risk patients following a normal 3-month protocol biopsy is effective in limiting acute rejection episodes and produces excellent rates of patient survival, graft function and complications.
在接受巴利昔单抗诱导治疗的肾移植受者中,包括早期停用类固醇在内的免疫抑制最小化的疗效和安全性尚不清楚。
这项回顾性队列研究报告了自2010年7月1日至2013年6月以来连续进行的298例肾移植的结果,这些移植采用巴利昔单抗诱导治疗,并对低免疫风险患者进行早期类固醇撤减,采用简单的免疫风险分层和3个月方案活检以优化治疗。该队列包括225例低风险患者(首次移植或HLA抗体计算反应频率(CRF≤50%且无供体特异性HLA抗体),他们接受了巴利昔单抗诱导治疗,在第7天停用类固醇,并使用他克莫司和霉酚酸酯(MMF)维持治疗,以及73例高风险患者,他们在最初3个月接受他克莫司、MMF和泼尼松龙治疗,随后长期使用他克莫司和泼尼松龙进行维持免疫抑制。未进行3个月方案活检的高风险患者继续接受三联免疫抑制治疗。
在接受IL2受体抗体诱导的低免疫风险受者中,可以安全地实现类固醇撤减。活检证实的急性排斥反应发生率在低风险组为15.1%,在高风险组为13.9%(包括在方案活检时检测到的亚临床排斥反应)。低风险组的1年移植存活率为93.3%,患者存活率为98.5%,高风险组分别为97.3%和100%。1年时每组的移植功能相似(低风险组平均eGFR为61.2±23.4 mL/min,高风险组为64.6±19.2 mL/min)。
对于低风险患者,采用巴利昔单抗诱导、他克莫司、MMF和泼尼松龙并早期停用类固醇,对于高风险患者在正常的3个月方案活检后停用MMF的免疫抑制方案,在限制急性排斥反应发作方面是有效的,并产生了优异的患者存活率、移植功能和并发症发生率。