Division of Gastroenterological Surgery, Saitama Medical University International Medical Center, Yamane, Hidaka-shi, Saitama, 350-1298, Japan.
World J Surg Oncol. 2020 Mar 11;18(1):54. doi: 10.1186/s12957-020-01818-7.
It is not clear whether stage II colon and rectal cancer have the same risk factors for recurrence. Thus, the purpose of this study was to identify the risk factors for postoperative recurrence in stage II colorectal cancer.
We retrospectively analyzed the data of 990 patients who had undergone radical surgery for stage II colorectal cancer. Patients' pathological features and characteristics including age, sex, family history, body mass index, tumor diameter, gross type of tumor, infiltration degree (T3/T4), tumor grade, perineural invasion, vascular invasion, lymphatic invasion, pathologic examination of lymph node number, and preoperative carcinoembryonic assay (CEA) level was compared between patients with and without recurrence. Finally, the prediction of the left and right colons was analyzed.
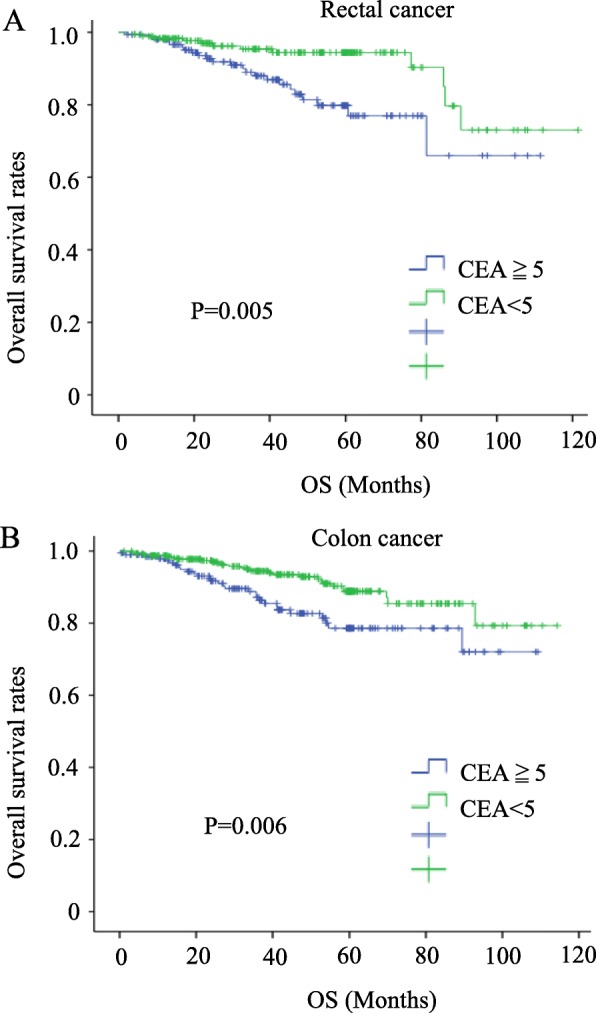
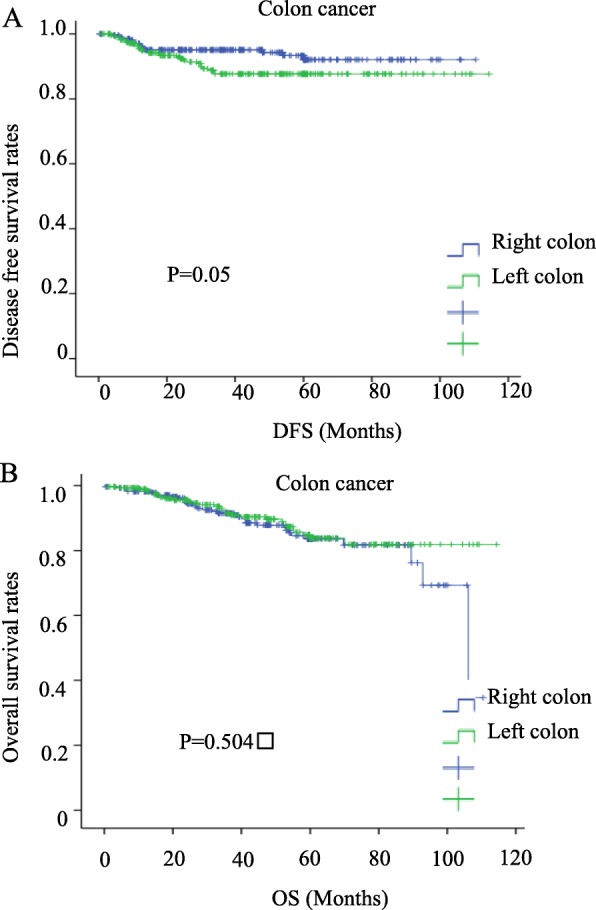
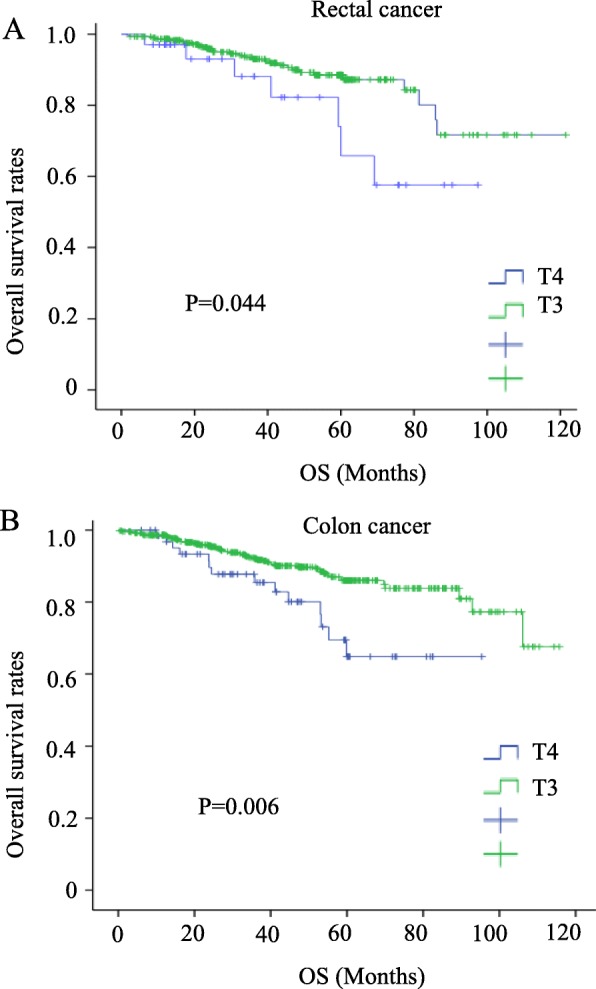
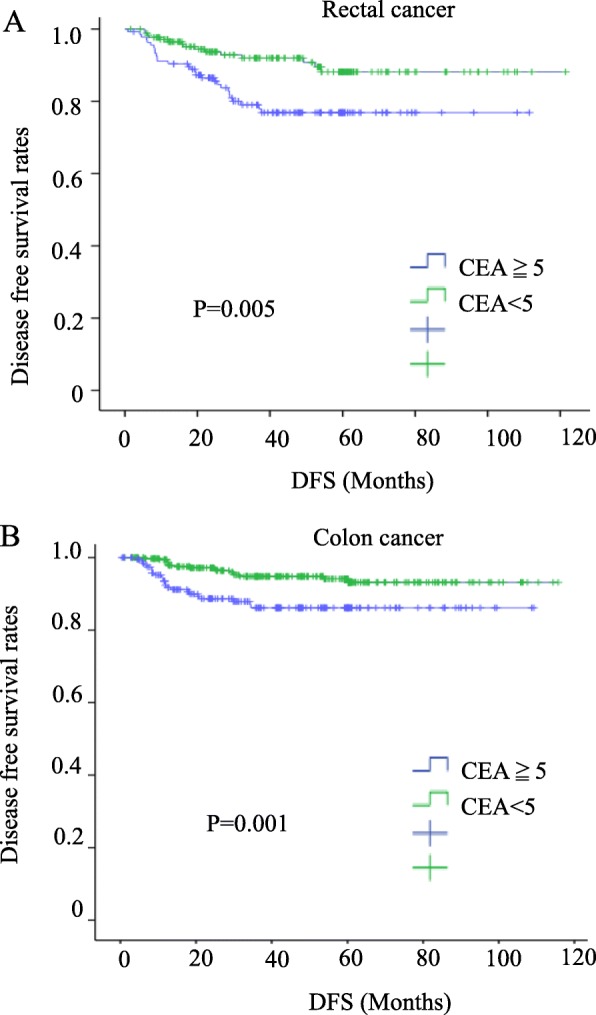
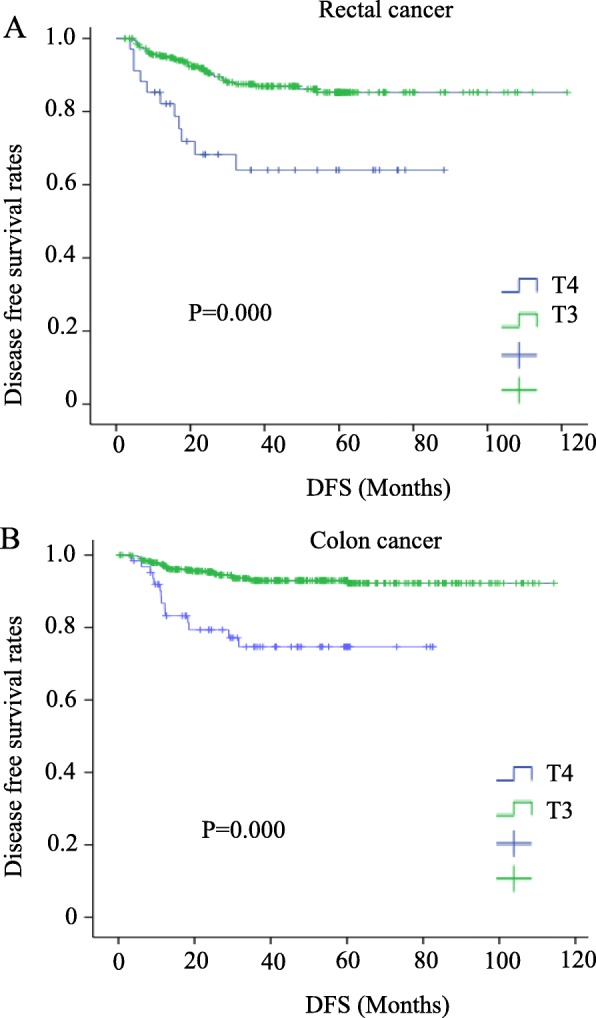
The mean ages of the colon cancer and rectal cancer patients were 69.5 years and 66.4 years, respectively. In total, 508 (82.1%) and 285 (76.8%) patients were treated laparoscopically for colon cancer and rectal cancer, respectively, with median follow-up periods of 42.2 months and 41.8 months, respectively. Forty-four recurrences occurred in both the colon cancer (7.1%) and rectal cancer (11.9%) groups. The preoperative serum CEA level and T4 infiltration were significantly higher in recurrent colorectal cancer patients. The postoperative recurrence rate of left colon cancer (descending colon, sigmoid colon) was higher than that of right colon cancer (cecum, ascending colon, transverse colon) (OR 2.191, 95% CI 1.091-4.400, P = 0.027). In COX survival factor analysis of colon cancer, the left colon is one of the independent risk factors (risk ratio 5.377, 95% CI 0.216-0.88, P = 0.02). In disease-free survival (DFS), the left colon has a relatively poor prognosis (P = 0.05). However, in the COX analysis and prognosis analysis of OS, no difference was found between the left colon and the right colon.
Preoperative CEA and depth of infiltration (T4) are high-risk factors associated with recurrence and are prognostic factors in stage II colorectal cancer. Left colon is also a risk factor for postoperative recurrence of stage II colon cancer.
目前尚不清楚 II 期结肠癌和直肠癌的复发风险因素是否相同。因此,本研究旨在确定 II 期结直肠癌术后复发的风险因素。
我们回顾性分析了 990 例接受 II 期结直肠癌根治性手术的患者资料。比较了患者的病理特征和特征,包括年龄、性别、家族史、体重指数、肿瘤直径、大体肿瘤类型、浸润程度(T3/T4)、肿瘤分级、神经周围侵犯、血管侵犯、淋巴血管侵犯、淋巴结病理检查数量以及术前癌胚抗原(CEA)水平,比较了有和无复发患者之间的差异。最后,分析了左、右结肠癌的预测情况。
结肠癌和直肠癌患者的平均年龄分别为 69.5 岁和 66.4 岁。508 例(82.1%)和 285 例(76.8%)结肠癌和直肠癌患者分别接受腹腔镜治疗,结肠癌和直肠癌的中位随访时间分别为 42.2 个月和 41.8 个月。结肠癌(7.1%)和直肠癌(11.9%)两组各有 44 例复发。复发结直肠癌患者术前血清 CEA 水平和 T4 浸润明显升高。左结肠癌(降结肠、乙状结肠)术后复发率高于右结肠癌(盲肠、升结肠、横结肠)(OR 2.191,95%CI 1.091-4.400,P=0.027)。在结肠癌 COX 生存因素分析中,左半结肠是独立危险因素之一(风险比 5.377,95%CI 0.216-0.88,P=0.02)。在无病生存(DFS)中,左半结肠的预后相对较差(P=0.05)。然而,在 COX 分析和 OS 预后分析中,左半结肠和右半结肠之间没有差异。
术前 CEA 和浸润深度(T4)是与复发相关的高危因素,也是 II 期结直肠癌的预后因素。左半结肠也是 II 期结肠癌术后复发的危险因素。