Department of Clinical Sciences, Institute of Tropical Medicine, Nationalestraat 155, Antwerpen, 2000, Belgium.
BMC Infect Dis. 2020 Mar 12;20(1):209. doi: 10.1186/s12879-020-4909-z.
Hepatitis C virus (HCV) infection is a major global health problem. WHO guidelines recommend screening all people living with HIV for hepatitis C. Considering the limited resources for health in low and middle income countries, targeted HCV screening is potentially a more feasible screening strategy for many HIV cohorts. Hence there is an interest in developing clinician-friendly tools for selecting subgroups of HIV patients for whom HCV testing should be prioritized. Several statistical methods have been developed to predict a binary outcome. Multiple studies have compared the performance of different predictive models, but results were inconsistent.
A cross-sectional HCV diagnostic study was conducted in the HIV cohort of Sihanouk Hospital Center of Hope in Phnom Penh, Cambodia. We compared the performance of logistic regression, Spiegelhalter-Knill-Jones and CART to predict Hepatitis C co-infection in this cohort. We estimated the number of HCV co-infections that would be missed. To correct for over-optimism, the leave-one-out bootstrap estimator was used for estimating this quantity.
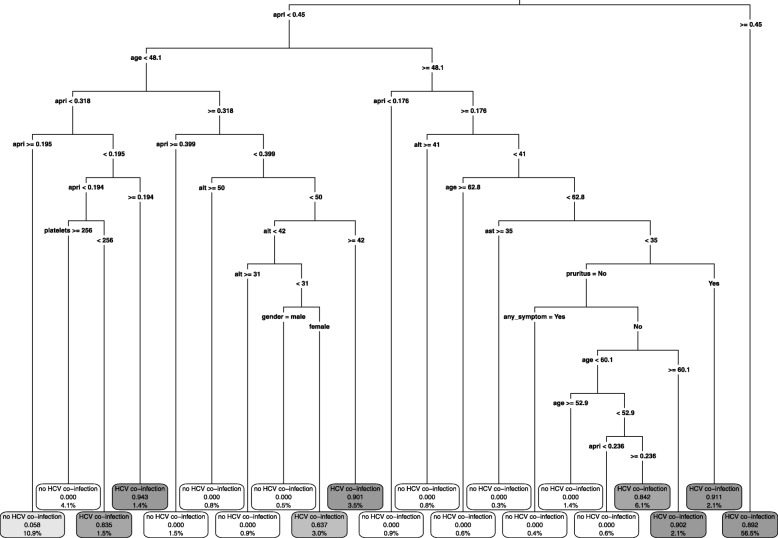
Logistic regression misses the fewest HCV co-infections (8%), but would still refer 98% of HIV patients for HCV testing. Spiegelhalter-Knill-Jones (SKJ) and CART respectively miss 12% and 29% of HCV co-infections but would only refer about 30% for HCV testing.
In our dataset, logistic regression has the highest log-likelihood and smallest proportions of HCV co-infections missed but Spiegelhalter-Knill-Jones has the highest area under the ROC curve. The likelihood ratios estimated by Spiegelhalter-Knill-Jones might be easier to interpret for clinicians than odds ratios estimated by logistic regression or the decision tree from CART. CART is the most flexible method, and no model has to be specified regarding presence of interactions and form of the relationship between outcome and predictor variables.
丙型肝炎病毒(HCV)感染是一个全球性的主要健康问题。世界卫生组织的指南建议对所有艾滋病毒感染者进行丙型肝炎筛查。考虑到中低收入国家的卫生资源有限,针对丙型肝炎的目标筛查可能是许多艾滋病毒队列更可行的筛查策略。因此,人们有兴趣开发适合临床医生的工具,以选择需要优先进行丙型肝炎检测的艾滋病毒患者亚组。已经开发了几种统计方法来预测二项结局。多项研究比较了不同预测模型的性能,但结果不一致。
在柬埔寨金边希望 Sihanouk 医院中心的艾滋病毒队列中进行了一项丙型肝炎诊断的横断面研究。我们比较了逻辑回归、Spiegelhalter-Knill-Jones 和 CART 在该队列中预测丙型肝炎合并感染的性能。我们估计了将错过的丙型肝炎合并感染数量。为了纠正过度乐观,使用留一法 bootstrap 估计量来估计这一数量。
逻辑回归错过的丙型肝炎合并感染最少(8%),但仍将 98%的艾滋病毒患者转诊进行丙型肝炎检测。Spiegelhalter-Knill-Jones(SKJ)和 CART 分别错过 12%和 29%的丙型肝炎合并感染,但仅将约 30%的患者转诊进行丙型肝炎检测。
在我们的数据集,逻辑回归具有最高的对数似然和最小的丙型肝炎合并感染漏诊比例,但 Spiegelhalter-Knill-Jones 具有最高的 ROC 曲线下面积。Spiegelhalter-Knill-Jones 估计的似然比可能比逻辑回归或 CART 的决策树估计的优势比更容易被临床医生解释。CART 是最灵活的方法,不必指定存在交互作用以及结局和预测变量之间的关系形式。