Institute of Epidemiology, Helmholtz Zentrum München-German Research Center for Environmental Health (GmbH), Ingolstädter Landstraße 1, 85764, Neuherberg, Germany.
German Center for Diabetes Research (DZD), München-Neuherberg, Germany.
Cardiovasc Diabetol. 2020 Mar 12;19(1):32. doi: 10.1186/s12933-020-01003-w.
Biomarkers may contribute to our understanding of the pathophysiology of various diseases. Type 2 diabetes (T2D) and coronary heart disease (CHD) share many clinical and lifestyle risk factors and several biomarkers are associated with both diseases. The current analysis aims to assess the relevance of biomarkers combined to pathway groups for the development of T2D and CHD in the same cohort.
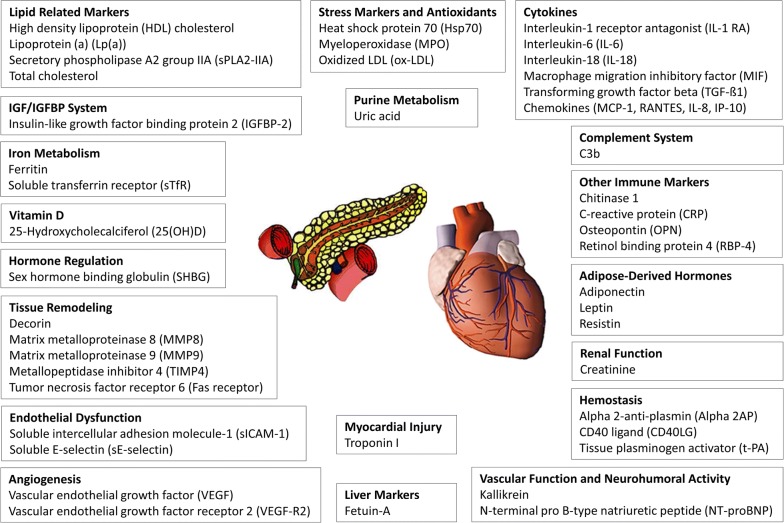
Forty-seven serum biomarkers were measured in the MONICA/KORA case-cohort study using clinical chemistry assays and ultrasensitive molecular counting technology. The T2D (CHD) analyses included 689 (568) incident cases and 1850 (2004) non-cases from three population-based surveys. At baseline, the study participants were 35-74 years old. The median follow-up was 14 years. We computed Cox regression models for each biomarker, adjusted for age, sex, and survey. Additionally, we assigned the biomarkers to 19 etiological pathways based on information from literature. One age-, sex-, and survey-controlled average variable was built for each pathway. We used the R coefficient of determination to assess the explained disease risk.
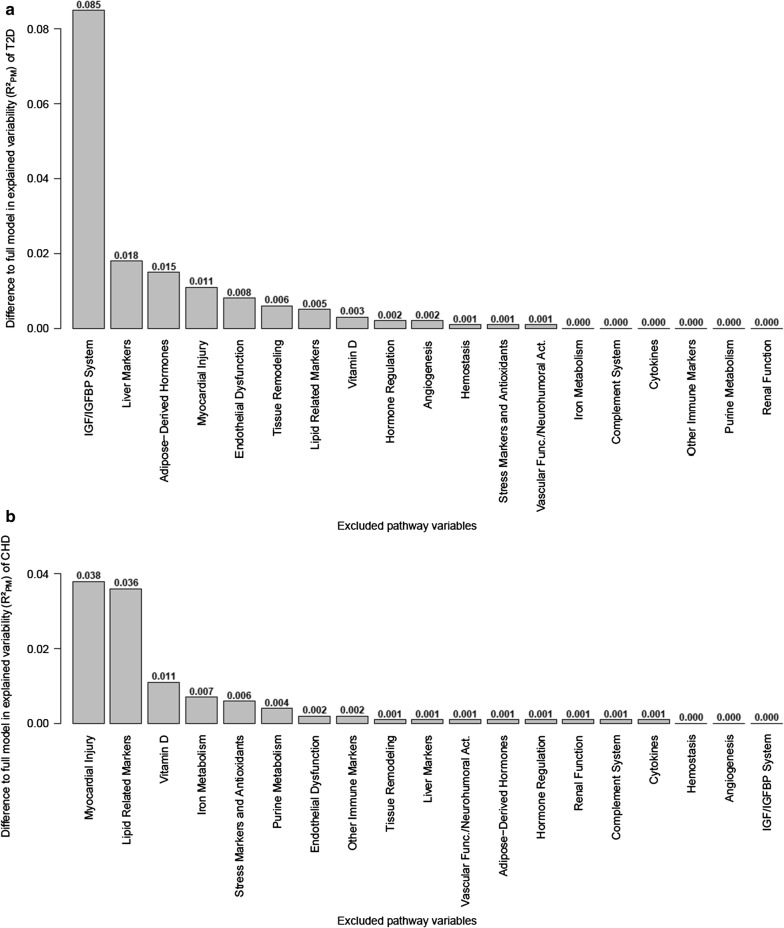
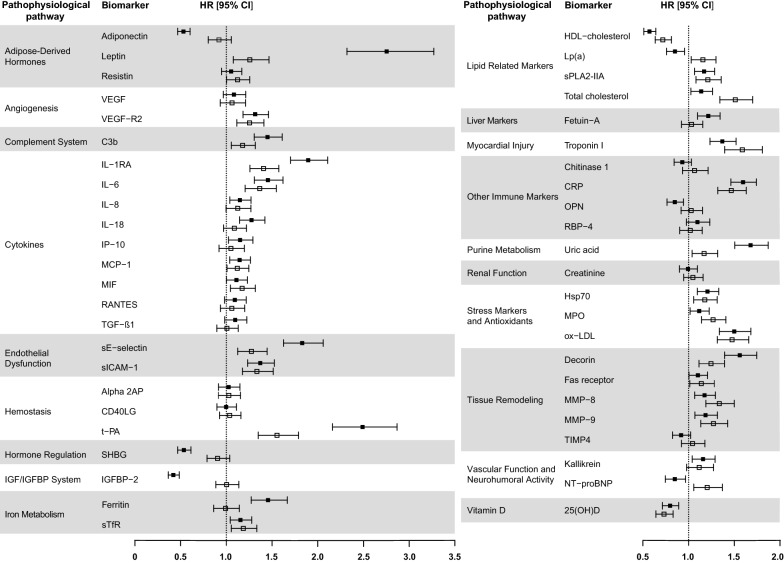
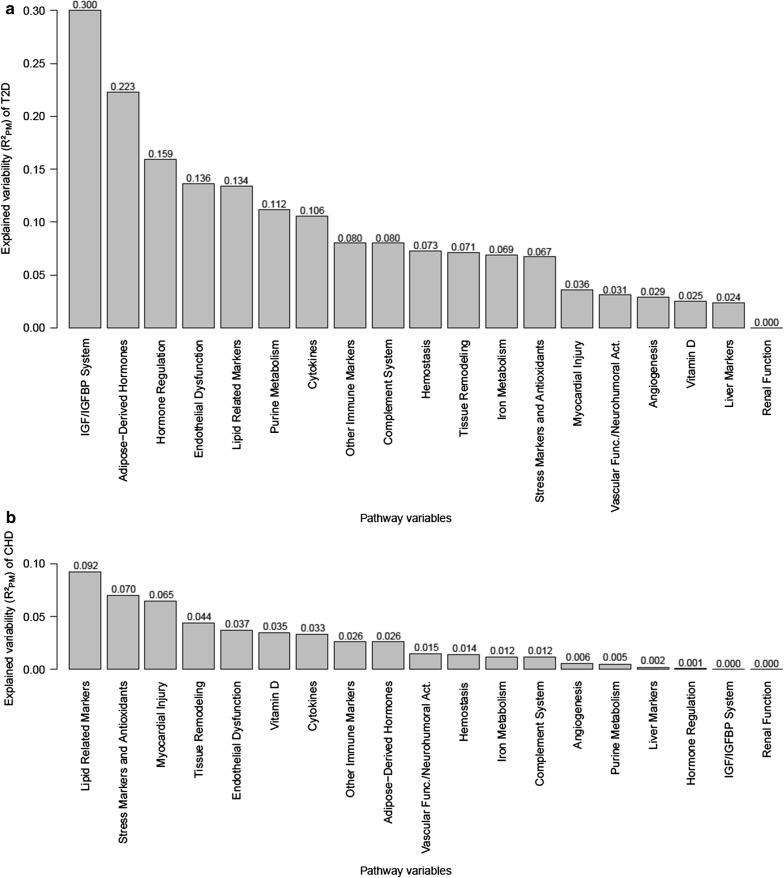
The associations of many biomarkers, such as several cytokines or the iron marker soluble transferrin receptor (sTfR), were similar in strength for T2D and CHD, but we also observed important differences. Lipoprotein (a) (Lp(a)) and N-terminal pro B-type natriuretic peptide (NT-proBNP) even demonstrated opposite effect directions. All pathway variables together explained 49% of the T2D risk and 21% of the CHD risk. The insulin-like growth factor binding protein 2 (IGFBP-2, IGF/IGFBP system pathway) best explained the T2D risk (about 9% explained risk, independent of all other pathway variables). For CHD, the myocardial-injury- and lipid-related-pathways were most important and both explained about 4% of the CHD risk.
The biomarker-derived pathway variables explained a higher proportion of the T2D risk compared to CHD. The ranking of the pathways differed between the two diseases, with the IGF/IGFBP-system-pathway being most strongly associated with T2D and the myocardial-injury- and lipid-related-pathways with CHD. Our results help to better understand the pathophysiology of the two diseases, with the ultimate goal of pointing out targets for lifestyle intervention and drug development to ideally prevent both T2D and CHD development.
生物标志物可能有助于我们理解各种疾病的病理生理学。2 型糖尿病(T2D)和冠心病(CHD)有许多共同的临床和生活方式危险因素,一些生物标志物与这两种疾病都有关联。本分析旨在评估同一队列中联合途径组的生物标志物对 T2D 和 CHD 发展的相关性。
使用临床化学分析和超灵敏分子计数技术,在 MONICA/KORA 病例-队列研究中测量了 47 种血清生物标志物。T2D(CHD)分析包括来自三项基于人群的调查的 689(568)例新发病例和 1850(2004)例非病例。在基线时,研究参与者年龄为 35-74 岁。中位随访时间为 14 年。我们为每个生物标志物计算了 Cox 回归模型,调整了年龄、性别和调查。此外,我们根据文献信息将生物标志物分配到 19 个病因途径。为每个途径构建了一个年龄、性别和调查控制的平均变量。我们使用 R 决定系数评估疾病风险的解释程度。
许多生物标志物(如几种细胞因子或铁标志物可溶性转铁蛋白受体(sTfR))与 T2D 和 CHD 的关联强度相似,但我们也观察到了重要的差异。脂蛋白(a)(Lp(a))和 N 端 pro B 型利钠肽(NT-proBNP)甚至表现出相反的作用方向。所有途径变量共同解释了 T2D 风险的 49%和 CHD 风险的 21%。胰岛素样生长因子结合蛋白 2(IGFBP-2,IGF/IGFBP 系统途径)最能解释 T2D 风险(约 9%的风险解释,独立于所有其他途径变量)。对于 CHD,心肌损伤和脂质相关途径最重要,两者都解释了 CHD 风险的约 4%。
与 CHD 相比,生物标志物衍生的途径变量解释了 T2D 风险的更高比例。两种疾病的途径排名不同,IGF/IGFBP 系统途径与 T2D 相关性最强,心肌损伤和脂质相关途径与 CHD 相关性最强。我们的研究结果有助于更好地理解这两种疾病的病理生理学,最终目标是指出生活方式干预和药物开发的目标,理想情况下可以预防 T2D 和 CHD 的发展。