Bottari Gabriella, Merli Pietro, Guzzo Isabella, Stoppa Francesca, Ruggeri Annalisa, Di Nardo Matteo, Del Bufalo Francesca, Galaverna Federica, Corrado Cecchetti, Locatelli Franco
Pediatric Intensive Care Unit, Department of Pediatric Anesthesia and Critical Care, Bambino Gesù, Children's Hospital, IRCSS, Rome, Italy.
Department of Pediatric Hematology and Oncology, Bambino Gesù, Children's Hospital, IRCSS, Rome, Italy.
Crit Care Explor. 2020 Jan 29;2(1):e0071. doi: 10.1097/CCE.0000000000000071. eCollection 2020 Jan.
To describe a pediatric case of cytokine release syndrome secondary to chimeric antigen receptor-modified T cells associated with acute respiratory distress syndrome.
Case report.
PICU.
A 14-year-old boy with refractory B cell precursor acute lymphoblastic leukemia given chimeric antigen receptor cells developed severe cytokine release syndrome 7 days after the drug product infusion with progressive respiratory failure. He was admitted to PICU with a clinical picture of acute respiratory distress syndrome, requiring mechanical ventilation, and secondary hemophagocytic lymphohistiocytosis.
Hemoadsorption with cartridge column (Cytosorb) in combination with continuous renal replacement therapy was associated to the anti-cytokine therapy (tocilizumab, a monoclonal antibody targeting interleukin-6 receptor).
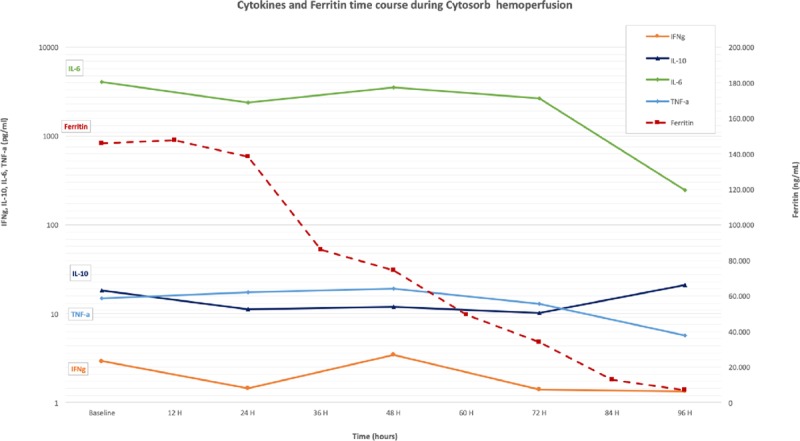
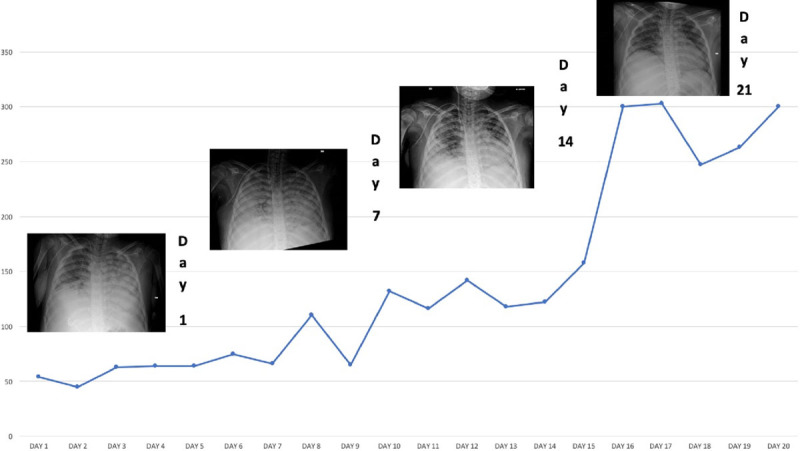
Decrease of the inflammatory biomarkers (ferritin, interleukin-6, interleukin-10) in the first 96 hours associated with a progressive improvement of acute respiratory distress syndrome (Pao/Fio ratio) 7 day after the start of the multimodal treatment.
This case suggests that hemoadsorption with cartridge column in combination with continuous renal replacement therapy and tocilizumab is safe and potentially effective in pediatric patients with severe cytokine release syndrome.
描述1例因嵌合抗原受体修饰T细胞继发细胞因子释放综合征并伴有急性呼吸窘迫综合征的儿科病例。
病例报告。
儿科重症监护病房。
一名14岁难治性B细胞前体急性淋巴细胞白血病男孩,在输注嵌合抗原受体细胞后7天出现严重细胞因子释放综合征,并伴有进行性呼吸衰竭。他因急性呼吸窘迫综合征临床表现入住儿科重症监护病房,需要机械通气,且继发噬血细胞性淋巴组织细胞增生症。
采用柱式血液吸附(Cytosorb)联合连续性肾脏替代治疗,并给予抗细胞因子治疗(托珠单抗,一种靶向白细胞介素-6受体的单克隆抗体)。
在多模式治疗开始后7天,前96小时内炎症生物标志物(铁蛋白、白细胞介素-6、白细胞介素-10)下降,同时急性呼吸窘迫综合征(氧合指数)逐渐改善。
该病例表明,柱式血液吸附联合连续性肾脏替代治疗及托珠单抗对于患有严重细胞因子释放综合征的儿科患者是安全且可能有效的。