Department of Environmental Health Sciences, Yale School of Public Health, 60 College Street, 4th Floor, Room 411, New Haven, CT, 06510, USA.
Collaboration for Research Integrity and Transparency (CRIT), Yale School of Medicine, New Haven, CT, 06510, USA.
BMC Med Res Methodol. 2020 Mar 14;20(1):64. doi: 10.1186/s12874-020-0914-6.
Among different investigators studying the same exposures and outcomes, there may be a lack of consensus about potential confounders that should be considered as matching, adjustment, or stratification variables in observational studies. Concerns have been raised that confounding factors may affect the results obtained for the alcohol-ischemic heart disease relationship, as well as their consistency and reproducibility across different studies. Therefore, we assessed how confounders are defined, operationalized, and discussed across individual studies evaluating the impact of alcohol on ischemic heart disease risk.
For observational studies included in a recent alcohol-ischemic heart disease meta-analysis, we identified all variables adjusted, matched, or stratified for in the largest reported multivariate model (i.e. potential confounders). We recorded how the variables were measured and grouped them into higher-level confounder domains. Abstracts and Discussion sections were then assessed to determine whether authors considered confounding when interpreting their study findings.
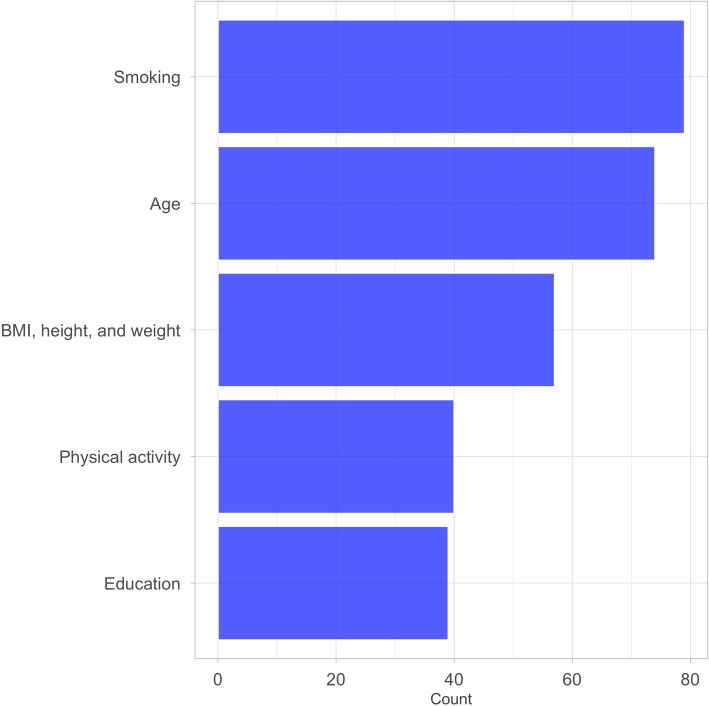
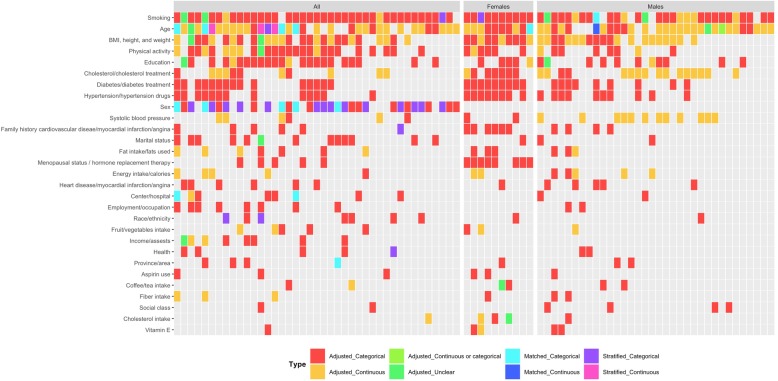
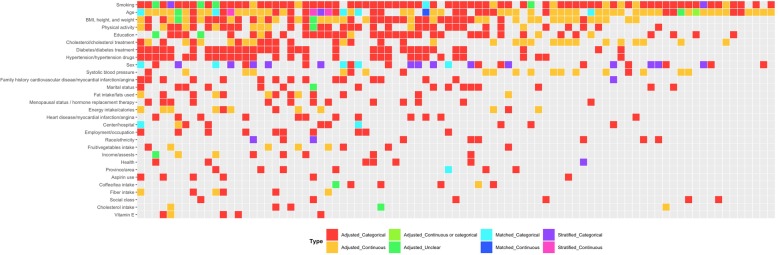
85 of 87 (97.7%) studies reported multivariate analyses for an alcohol-ischemic heart disease relationship. The most common higher-level confounder domains included were smoking (79, 92.9%), age (74, 87.1%), and BMI, height, and/or weight (57, 67.1%). However, no two models adjusted, matched, or stratified for the same higher-level confounder domains. Most (74/87, 85.1%) articles mentioned or alluded to "confounding" in their Abstract or Discussion sections, but only one stated that their main findings were likely to be affected by residual confounding. There were five (5/87, 5.7%) authors that explicitly asked for caution when interpreting results.
There is large variation in the confounders considered across observational studies evaluating the impact of alcohol on ischemic heart disease risk and almost all studies spuriously ignore or eventually dismiss confounding in their conclusions. Given that study results and interpretations may be affected by the mix of potential confounders included within multivariate models, efforts are necessary to standardize approaches for selecting and accounting for confounders in observational studies.
在研究相同暴露和结局的不同研究者中,对于应该作为匹配、调整或分层变量纳入观察性研究的潜在混杂因素,可能缺乏共识。有人担心,混杂因素可能会影响到关于酒精与缺血性心脏病关系的研究结果,以及这些结果在不同研究中的一致性和可重复性。因此,我们评估了在评估酒精对缺血性心脏病风险影响的个体研究中,混杂因素是如何被定义、操作和讨论的。
在最近的一项酒精与缺血性心脏病荟萃分析中,我们对纳入的观察性研究确定了在最大报告的多变量模型中进行调整、匹配或分层的所有变量(即潜在混杂因素)。我们记录了变量的测量方式,并将它们归入更高层次的混杂因素领域。然后评估摘要和讨论部分,以确定作者在解释研究结果时是否考虑了混杂因素。
87 项研究中有 85 项(97.7%)报告了与酒精与缺血性心脏病关系的多变量分析。最常见的更高层次的混杂因素领域包括吸烟(79 项,92.9%)、年龄(74 项,87.1%)和 BMI、身高和/或体重(57 项,67.1%)。然而,没有两个模型调整、匹配或分层的是相同的更高层次的混杂因素领域。大多数(74/87,85.1%)文章在摘要或讨论部分提到或暗示了“混杂”,但只有一篇文章表示他们的主要发现可能受到残余混杂的影响。有 5 位(5/87,5.7%)作者明确要求在解释结果时要谨慎。
评估酒精对缺血性心脏病风险影响的观察性研究中,考虑的混杂因素存在很大差异,几乎所有研究都在其结论中有意或无意地忽略或最终否定混杂因素的影响。鉴于研究结果和解释可能受到纳入多变量模型中的潜在混杂因素组合的影响,有必要努力标准化在观察性研究中选择和考虑混杂因素的方法。