Guha Avirup, Dey Amit Kumar, Omer Shuab, Abraham William T, Attizzani Guilherme, Jneid Hani, Addison Daniel
Cardio-Oncology Program, Division of Cardiology, Ohio State University, Columbus, Ohio; Harrington Heart and Vascular Institute, Case Western Reserve University, Cleveland, Ohio.
National Heart, Lung and Blood Institute, Bethesda, Maryland.
Am J Cardiol. 2020 May 1;125(9):1355-1360. doi: 10.1016/j.amjcard.2020.01.047. Epub 2020 Feb 8.
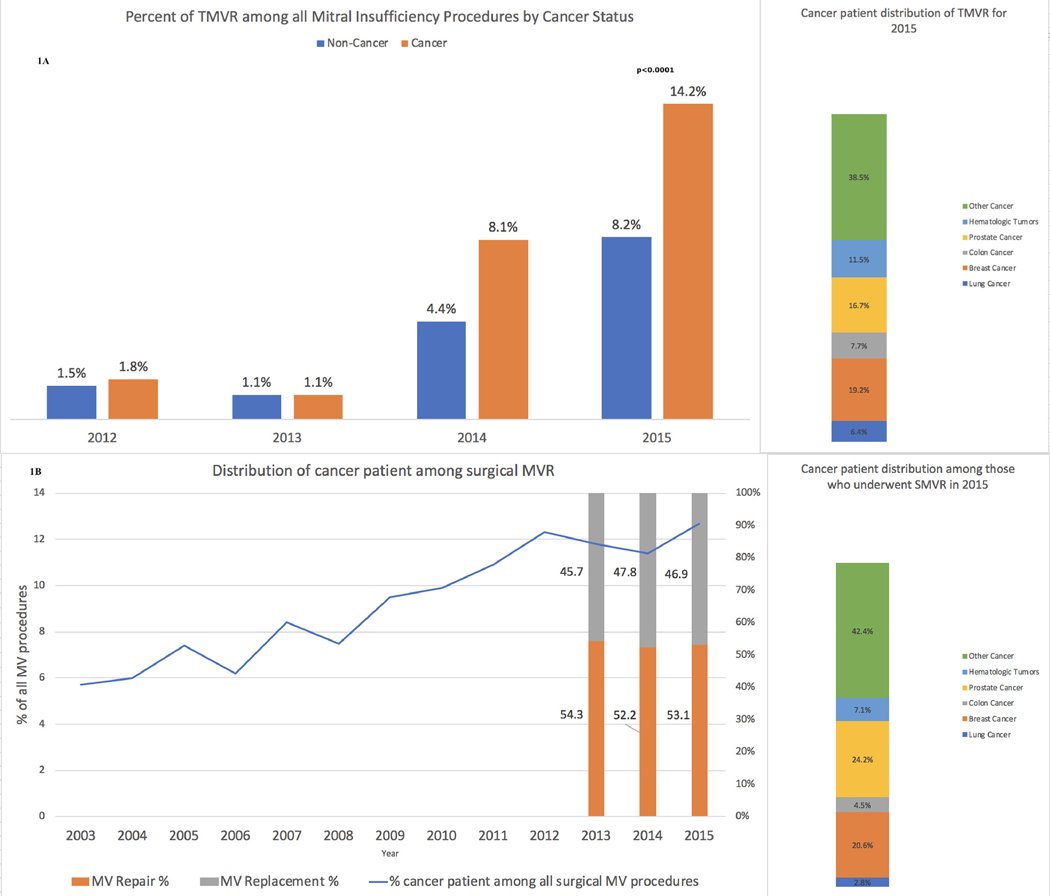
In the era of emerging options for mitral valvular intervention, we sought to characterize the relative utilization, outcomes, and posthospital dispositions of patients referred for transcatheter mitral valve repair (TMVRepair) and surgical mitral valve procedures (SMVP), by cancer-status. Leveraging the National Inpatient Sample, a representative national dataset, ICD-9 codes for all adults >18 years with co-morbid mitral regurgitation, and cancer without metastatic disease admitted from 2003 to 2015 were queried. TMVRepair was performed in 700 hospitalizations from 2012 to 2015, whereas SMVP was utilized during 12,863 hospitalizations from 2003 to 2015. During follow-up, we observed a proportional increase in TMVRepair utilization among cancer patients (vs noncancer), particularly in 2015 (14.2% vs 8.2%, p <0.0001). There was no difference in in-hospital mortality (1.4% vs 1.8%, p = 0.71), ischemic stroke (0.7% vs 0.6%, p = 0.97), major bleeding (8.6% vs 10.9%, p = 0.36), and home discharge (62.1% vs 65.7%, p = 0.45) by cancer-status among patients who underwent TMVRepair; but, cost of care was increased ($52,325 vs $48,832, p <0.0001). Similarly, there was no difference in in-hospital mortality (3.1% vs 3.4%, p = 0.36), ischemic stroke (2.6% vs 3.1%, p = 0.16) as well as the cost-of-care ($58,106 vs $58,844, p = 0.49) among those who underwent SMVP across the same period; but, cancer was associated with increased major bleeding (34.9% vs 30.5%, p <0.0001), and lower likelihood of home discharge (32.8% vs 38.6%, p <0.0001). In conclusion, TMVRepair and SMVP were associated with comparable in-hospital mortality and outcomes in cancer versus noncancer patients. However, cancer patients treated with SMVP experienced more frequent bleeding related complications compared with noncancer patients.
在二尖瓣介入治疗新选择不断涌现的时代,我们试图按癌症状态,对接受经导管二尖瓣修复术(TMVRepair)和二尖瓣手术(SMVP)患者的相对利用率、治疗结果及出院后去向进行特征分析。利用具有全国代表性的国家住院患者样本数据集,查询了2003年至2015年所有年龄大于18岁、合并二尖瓣反流且无转移性疾病的癌症成年患者的ICD - 9编码。2012年至2015年期间,有700例住院患者接受了TMVRepair,而2003年至2015年期间,有12,863例住院患者接受了SMVP。在随访期间,我们观察到癌症患者(与非癌症患者相比)中TMVRepair的利用率呈比例增加,尤其是在2015年(14.2%对8.2%,p<0.0001)。接受TMVRepair的患者中,按癌症状态划分,住院死亡率(1.4%对1.8%,p = 0.71)、缺血性卒中(0.7%对0.6%,p = 0.97)、大出血(8.6%对10.9%,p = 0.36)以及出院回家比例(62.1%对65.7%,p = 0.45)均无差异;但是,护理费用有所增加(52,325美元对48,832美元,p<0.0001)。同样,同期接受SMVP的患者中,住院死亡率(3.1%对3.4%,p = 0.36)、缺血性卒中(2.6%对3.1%,p = 0.16)以及护理费用(58,106美元对58,844美元,p = 0.49)均无差异;但是,癌症与大出血增加相关(34.9%对30.5%,p<0.0001),且出院回家的可能性较低(32.8%对38.6%,p<0.0001)。总之,TMVRepair和SMVP在癌症患者与非癌症患者中的住院死亡率及治疗结果相当。然而,与非癌症患者相比,接受SMVP治疗的癌症患者出血相关并发症更频繁。