Department of Radiation Oncology, The First Affiliated Hospital of Xiamen University, Teaching Hospital of Fujian Medical University, Xiamen, 361003, PR China.
Department of Obstetrics and Gynecology, The First Affiliated Hospital of Xiamen University, Teaching Hospital of Fujian Medical University, Xiamen, PR China.
Breast. 2020 Jun;51:2-10. doi: 10.1016/j.breast.2020.02.012. Epub 2020 Mar 3.
The 8th edition of the American Joint Committee on Cancer (AJCC) pathological staging system for breast cancer considers biologic factors in addition to the anatomical features included in the previous systems. The purpose of this study was to determine the validity of the 8th AJCC staging system for T1-2N1 breast cancer and to assess the effect of additional chemotherapy and radiotherapy according to the new pathologic stages.
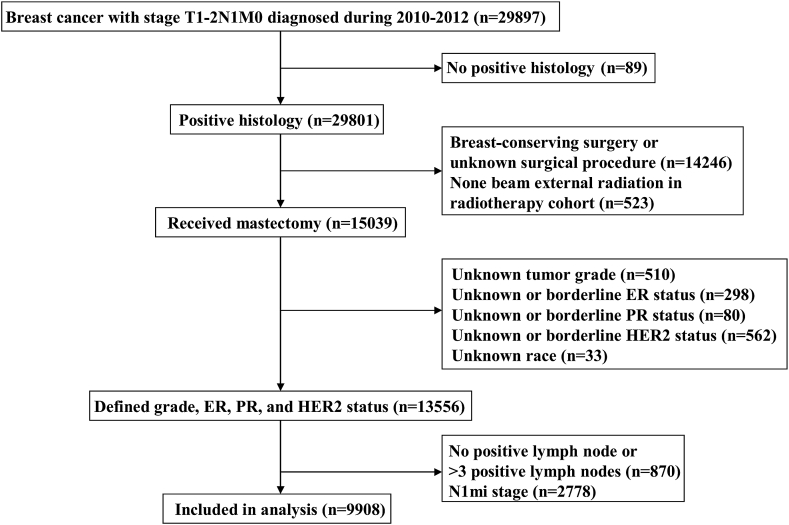
The cohort included patients from the Surveillance, Epidemiology, and End Results program (2010-2012) who had stage T1-2N1 invasive breast carcinoma and underwent mastectomy. All patients were restaged using the 8th AJCC staging system. The Kaplan-Meier method, Cox proportional hazards regression, and competing risks models were used for data analysis.
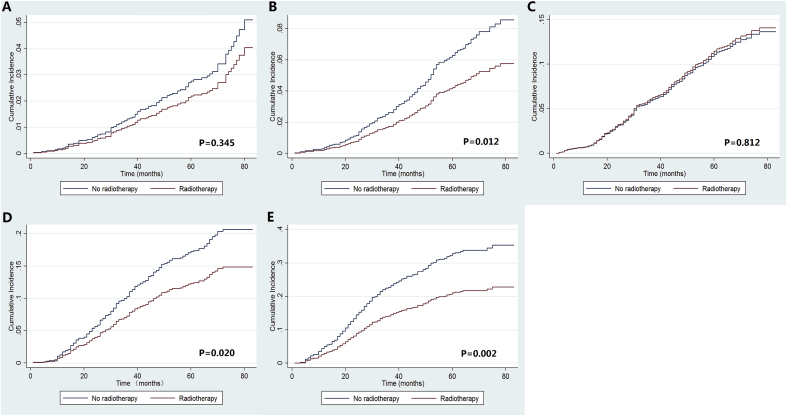
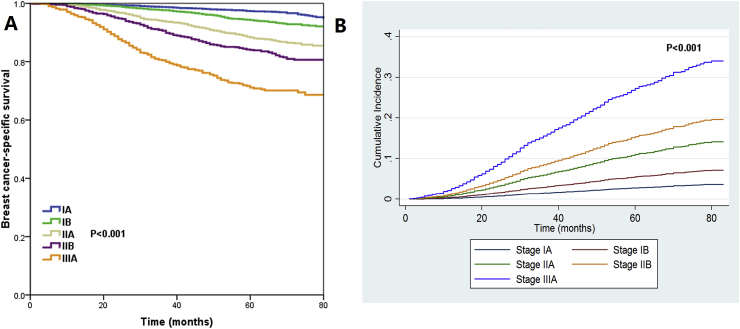
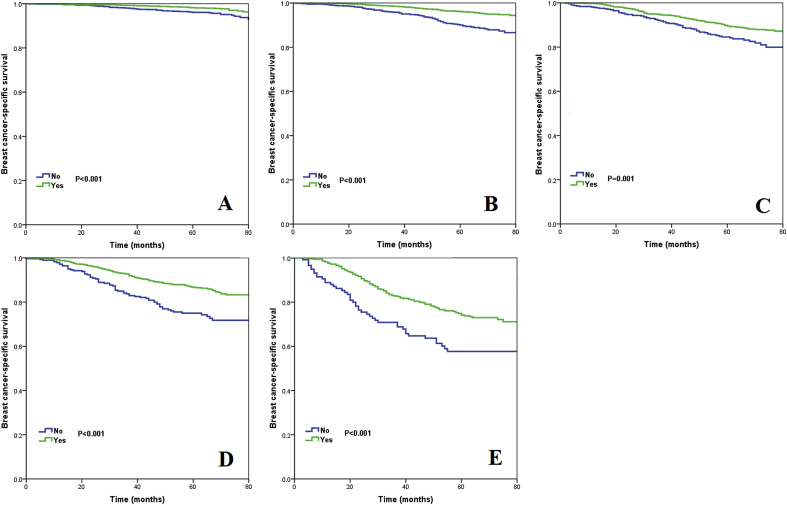
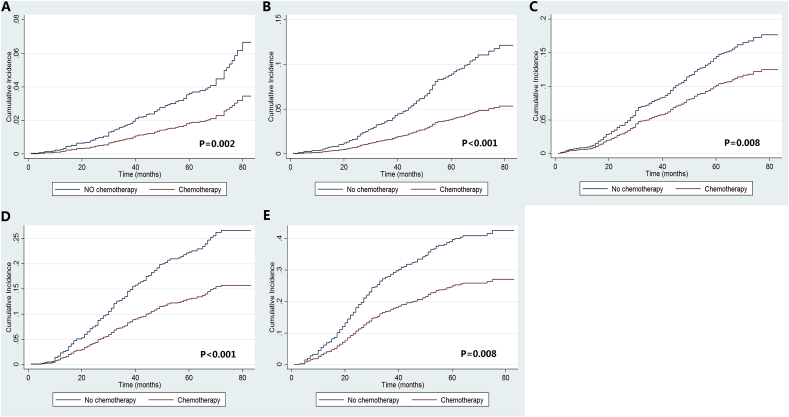
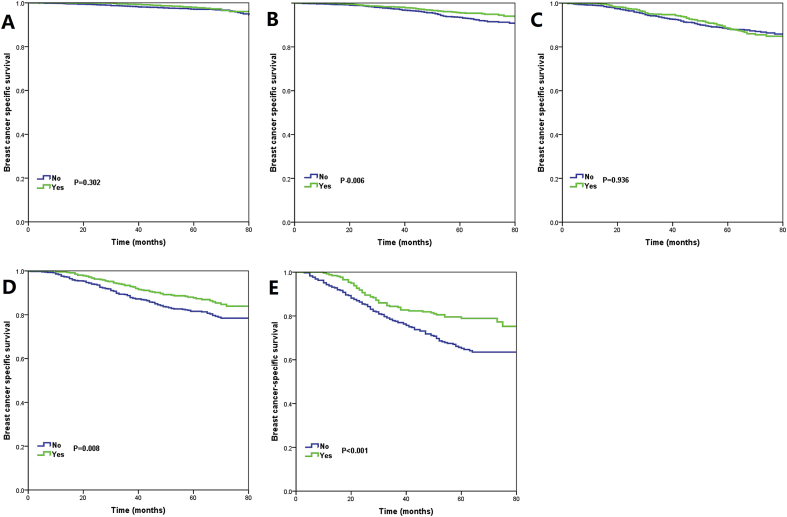
We identified 9908 patients including 3022 (30.5%), 3131 (31.6%), 1940 (19.6%), 1194 (12.1%), and 621 (6.3%) were classified with stage IA, IB, IIA, IIB, and IIIA disease, respectively. The 5-year breast cancer-specific survival (BCSS) was 97.3%, 94.3%, 88.3%, 84.0%, and 71.1% for stage IA, IB, IIA, IIB, and IIIA disease, respectively. Higher pathological stage was associated with a significantly higher risk of breast cancer-related death. Chemotherapy was associated with better BCSS regardless of the pathological stage, but radiotherapy was only associated with better BCSS in stage IIIA disease.
The 8th AJCC pathological staging system provides more refined stratification for T1-2N1 breast cancer patients after mastectomy and may meet the needs of the current trend of individualized decision making for chemotherapy and radiotherapy in this patient subset.
第 8 版美国癌症联合委员会(AJCC)乳腺癌病理分期系统除了包含之前系统中的解剖特征外,还考虑了生物学因素。本研究旨在确定第 8 版 AJCC 分期系统对 T1-2N1 乳腺癌的有效性,并根据新的病理分期评估额外化疗和放疗的效果。
该队列纳入了来自监测、流行病学和最终结果计划(2010-2012 年)的患者,这些患者患有 T1-2N1 浸润性乳腺癌并接受了乳房切除术。所有患者均采用第 8 版 AJCC 分期系统进行重新分期。采用 Kaplan-Meier 方法、Cox 比例风险回归和竞争风险模型进行数据分析。
我们共纳入了 9908 例患者,其中 3022 例(30.5%)、3131 例(31.6%)、1940 例(19.6%)、1194 例(12.1%)和 621 例(6.3%)分别被归类为 IA、IB、IIA、IIB 和 IIIA 期疾病。IA、IB、IIA、IIB 和 IIIA 期疾病的 5 年乳腺癌特异性生存率(BCSS)分别为 97.3%、94.3%、88.3%、84.0%和 71.1%。较高的病理分期与乳腺癌相关死亡的风险显著增加相关。化疗与更好的 BCSS 相关,无论病理分期如何,但放疗仅与 IIIA 期疾病的 BCSS 相关。
第 8 版 AJCC 病理分期系统为接受乳房切除术的 T1-2N1 乳腺癌患者提供了更精细的分层,可能满足当前该患者亚组化疗和放疗个体化决策的趋势需求。