Department of Interventional and Diagnostic Radiology, University of Leipzig - Heart Center, Struempellstrasse 39, 04289, Leipzig, Germany.
Cardiovascular Imaging Research Center, Massachusetts General Hospital - Harvard Medical School, Boston, MA, USA.
Eur Radiol. 2020 Aug;30(8):4317-4326. doi: 10.1007/s00330-019-06653-3. Epub 2020 Mar 16.
To associate coronary wall volume and composition, derived from coronary computed tomography angiography (CTA), with cardiac allograft vasculopathy (CAV) detected on invasive coronary angiography (ICA) in heart-transplanted (HTX) patients.
We included consecutive adults who received ICA and coronary CTA for evaluation of CAV ≥ 10 months after HTX. In all coronary segments, we assessed lumen and wall volumes and segmental length, calculated volume-length ratio (VLR) (volumes indexed by segmental length; mm/mm), wall burden (WB) (wall/wall + lumen volumes; %), and assessed proportions of calcified, fibrotic, fibro-fatty, and low-attenuation tissue (%) in coronary wall. We rendered independent CTA measures associated with CAV by ICA, tested their discriminatory capacity, and assessed concordance between CTA and ICA.
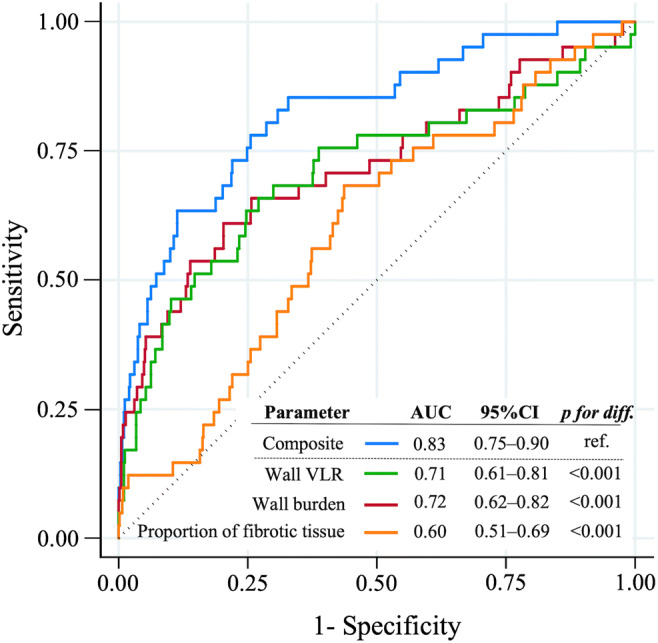
Among 50 patients (84% men; 53.6 ± 11.9 years), we analyzed 632 coronary segments. Mean interval between HTX and CTA was 6.7 ± 4.7 years and between ICA and CTA 1 (0-1) day. Segmental VLR, WB, and proportion of fibrotic tissue were independently associated with CAV (OR = 1.06-1.27; p ≤ 0.002), reaching a high discriminatory capacity (combination of all three: AUC = 0.84; 95%CI, 0.75-0.90). Concordance between CTA and ICA was higher in advanced CAV (88%) compared with that in none (37%) and mild (19%) CAV. Discordance was primarily driven by a large number of segments with coronary wall changes on CTA but without luminal stenoses on ICA (177/591; 25%).
CTA-derived coronary wall VLR, WB, and the proportion of fibrotic tissue are independent markers of CAV. Combination of these three parameters may aid the detection of early CAV not detected by ICA, the current standard of care.
• Coronary CTA detects CAV in HTX patients. • Coronary wall volume-length ratio, wall burden, and proportion of fibrotic tissue are independently associated with CAV. • In contrast to ICA, coronary CTA may identify the early stages of CAV.
通过冠状动脉计算机断层血管造影(CTA)检测到的冠状动脉壁体积和成分,与心脏移植(HTX)患者经侵入性冠状动脉造影(ICA)检测到的心脏移植物血管病(CAV)相关联。
我们纳入了连续接受 ICA 和冠状动脉 CTA 评估的成年人,这些患者在 HTX 后至少 10 个月接受了 CAV 评估。在所有冠状动脉节段中,我们评估了管腔和壁体积以及节段长度,计算了体积长度比(VLR)(以节段长度为指标的体积;mm/mm)、壁负荷(WB)(壁/壁+管腔体积;%),并评估了冠状动脉壁中钙化、纤维化、纤维脂肪和低衰减组织的比例(%)。我们评估了与 ICA 相关的独立 CTA 指标,并测试了它们的区分能力,评估了 CTA 和 ICA 之间的一致性。
在 50 名患者(84%为男性;53.6±11.9 岁)中,我们分析了 632 个冠状动脉节段。HTX 和 CTA 之间的平均间隔时间为 6.7±4.7 年,ICA 和 CTA 之间的平均间隔时间为 1(0-1)天。节段 VLR、WB 和纤维组织比例与 CAV 独立相关(OR=1.06-1.27;p≤0.002),具有较高的区分能力(所有三种参数的组合:AUC=0.84;95%CI,0.75-0.90)。与无(37%)和轻度(19%)CAV 相比,CTA 和 ICA 之间的一致性在晚期 CAV(88%)中更高。不一致主要是由于 CTA 上存在大量冠状动脉壁变化但 ICA 上无管腔狭窄的节段(177/591;25%)。
CTA 衍生的冠状动脉壁 VLR、WB 和纤维化组织比例是 CAV 的独立标志物。这三个参数的组合可能有助于检测 ICA 无法检测到的早期 CAV,后者是目前的护理标准。
• CTA 可检测 HTX 患者的 CAV。• 冠状动脉壁体积长度比、壁负荷和纤维化比例与 CAV 独立相关。• 与 ICA 相比,冠状动脉 CTA 可能识别 CAV 的早期阶段。