Schiaroli Elisabetta, De Socio Giuseppe Vittorio, Gabrielli Chiara, Papalini Chiara, Nofri Marco, Baldelli Franco, Francisci Daniela
Clinic of Infectious Diseases, Department of Medicine, University of Perugia, Perugia, Italy.
Mediterr J Hematol Infect Dis. 2020 Mar 1;12(1):e2020017. doi: 10.4084/MJHID.2020.017. eCollection 2020.
Despite progress in the prevention and treatment of HIV, persistent issues concerning the evaluation of continuum in care from the serological diagnosis to virologic success remains. Considering the 2020 UNAIDS target 90-90-90 for diagnosis, treatment, and viral suppression of people living with HIV (PLWH), our purpose was to verify if, starting from new diagnoses, the viral suppression rate of our cohort of new PLWH satisfied the second and the third steps.
This retrospective study regards all patients aged ≥15 undergoing HIV test at our clinic between January 2005 and December 2017. We evaluated the second and the third '90 UNAIDS targets and the unclaimed tests, linkage to care, retention in ART, and the viral suppression at 1 and 2 years. Logistic regression (odds ratio, 95% confidence interval) was performed.
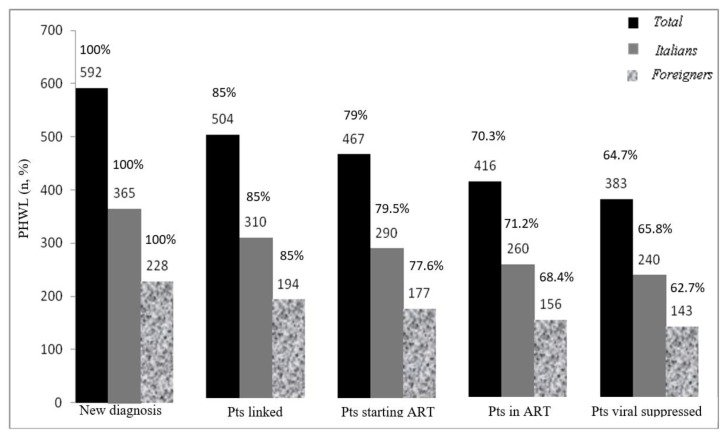
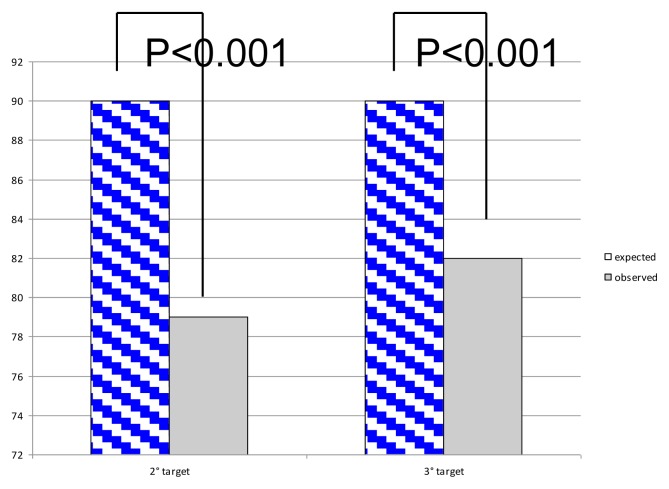
We observed 592 new diagnoses for HIV infection: 61.4% on Italians, 38.5% on foreigners. An antiretroviral treatment was started on 78.8% of the new diagnoses (467/592) (second UNAIDS target), and a viral suppression was obtained at 2 years on 82% of PLWH who had started ART (383/467) (third UNAIDS target), namely only 64.7% of the new diagnoses instead of the hoped-for 81% of the UNAIDS target. Logistic regressions demonstrated that second and third '90 UNAIDS targets were unrelated to sex, nationality, CD4 cells count, HIV-RNA and CDC stage (p>0.05). The age class 25-50 years (OR=2.24; 95% CI = 1.06-4.37; p=0.04) achieves more likely viral suppression when compared with patients <25 years. Considering the continuum of care, 88 (15%) PLWH were lost to engagement in care (55 unclaimed tests and 33 unlinked to care), 37 didn't start ART, 51 were LFTU at 2 years.
UNAIDS goal was far to be reached. The main challenges were unreturned tests as well as the retention in ART. Rapid tests for a test-treat strategy and frequent phone communications in the first ART years could facilitate UNAIDS target achievement.
尽管在艾滋病毒的预防和治疗方面取得了进展,但从血清学诊断到病毒学成功的连续护理评估方面仍存在持续问题。考虑到2020年联合国艾滋病规划署关于艾滋病毒感染者(PLWH)诊断、治疗和病毒抑制的90-90-90目标,我们的目的是验证从新诊断开始,我们的新PLWH队列的病毒抑制率是否满足第二步和第三步。
这项回顾性研究涉及2005年1月至2017年12月期间在我们诊所接受艾滋病毒检测的所有年龄≥15岁的患者。我们评估了联合国艾滋病规划署的第二个和第三个“90”目标以及未领取的检测、与护理的联系、抗逆转录病毒治疗的保留率以及1年和2年时的病毒抑制情况。进行了逻辑回归(比值比,95%置信区间)。
我们观察到592例新的艾滋病毒感染诊断:61.4%为意大利人,38.5%为外国人。78.8%的新诊断患者(467/592)开始了抗逆转录病毒治疗(联合国艾滋病规划署第二个目标),在开始抗逆转录病毒治疗的PLWH中,82%(383/467)在2年时实现了病毒抑制(联合国艾滋病规划署第三个目标),即仅占新诊断患者的64.7%,而非联合国艾滋病规划署目标所期望的81%。逻辑回归表明,联合国艾滋病规划署的第二个和第三个“90”目标与性别、国籍、CD4细胞计数、HIV-RNA和疾病控制中心阶段无关(p>0.05)。与<25岁的患者相比,25-50岁年龄组(OR=2.24;95%CI = 1.06-4.37;p=0.04)更有可能实现病毒抑制。考虑到连续护理,88例(15%)PLWH失去了与护理的联系(55例未领取检测,33例与护理无关联),37例未开始抗逆转录病毒治疗,51例在2年时治疗失败。
联合国艾滋病规划署的目标远未实现。主要挑战是检测未返还以及抗逆转录病毒治疗的保留率。采用检测即治疗策略的快速检测以及在抗逆转录病毒治疗的头几年频繁进行电话沟通可能有助于实现联合国艾滋病规划署的目标。