Kok Victor C
Department of Medical Oncology, Kuang Tien General Hospital Cancer Center, Taichung, Taiwan.
Department of Bioinformatics and Medical Engineering, Asia University Taiwan, Taichung, Taiwan.
Front Oncol. 2020 Feb 28;10:268. doi: 10.3389/fonc.2020.00268. eCollection 2020.
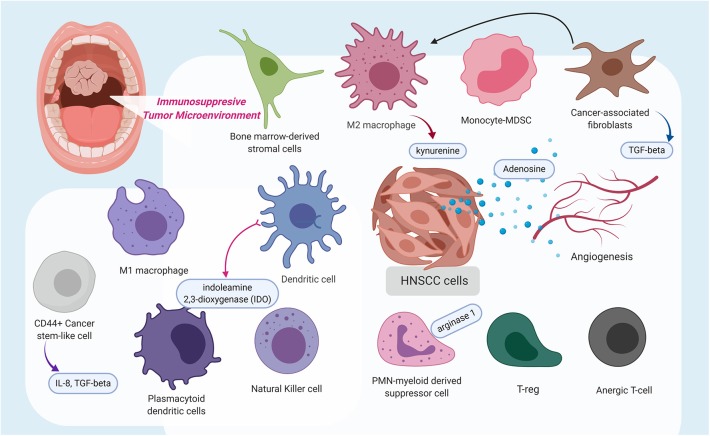
Starting in 2014, large phase III clinical trials began to disclose the study results of using programmed death (PD)-1 immune checkpoint inhibitors (ICIs) (pembrolizumab, nivolumab) and PD-ligand (L)1 (atezolizumab, durvalumab, avelumab) ICIs immunotherapy in patients with advanced head and neck squamous cell carcinoma (HNSCC). In the recurrent and metastatic (R/M), cisplatin-refractory setting, nivolumab achieved a 2.2-fold increase of the median 1-year overall survival as compared with investigators' choice of salvage chemotherapy (36.0 vs. 16.6%). A paradigm shift to the winning regimen, pembrolizumab combined with platinum and infusional fluorouracil, has outperformed the past gold standard of cetuximab-based platinum and fluorouracil combination in terms of overall survival (median, 13.6 vs. 10.1 mo) when administered as the first-line treatment for R/M HNSCC. Nevertheless, many patients still did not respond to the PD-1/PD-L1 checkpoint inhibitor treatment, indicating innate, adapted, or quickly acquired resistance to the immunotherapy. The mechanisms of resistance to ICIs targeting the PD-1/PD-L1 signaling pathway in the context of HNSCC are the focus of this review. The past 5 years have seen improved understanding of the mechanisms underlying checkpoint inhibition resistance in tumor cells, such as: tumor cell adaption with malfunction of the antigen-presenting machinery via class I human leukocyte antigen (HLA), reintroduction of cyclin D-cyclin-dependent kinase (CDK) 4 complex to cell cycles, enrichment of CD44+ cancer stem-like cells, or development of inactivating mutation in IKZF1 gene; impairment of T-cell functions and proliferation through mutations in the interferon-γ-regulating genes, suppression of the stimulator of interferon genes (STING) pathway, or resulted from constitutional nutritional iron deficiency state; metabolic reprogramming by cancer cells with changes in metabolites such as GTP cyclohydrolase 1, tetrahydrobiopterin, kynurenine, indoleamine 2,3-dioxygenase, and arginase 1; defective dendritic cells, CD-69 sufficient state; and the upregulation or activation of the alternative immune checkpoints, including lymphocyte activation gene-3 (LAG3), T-cell immunoglobulin and ITIM domain (TIGIT)/CD155 pathway, T-cell immunoglobulin mucin-3 (TIM-3), and V domain-containing Ig suppressor of T-cell activation (VISTA). Several potential biomarkers or biosignatures, which could predict the response or resistance to the PD-1/PD-L1 checkpoint immunotherapy, are also discussed.
从2014年开始,大型III期临床试验陆续公布了使用程序性死亡(PD)-1免疫检查点抑制剂(ICI)(帕博利珠单抗、纳武利尤单抗)以及PD配体(L)1(阿替利珠单抗、度伐利尤单抗、阿维鲁单抗)ICI免疫疗法治疗晚期头颈部鳞状细胞癌(HNSCC)患者的研究结果。在复发和转移性(R/M)、顺铂难治性的情况下,与研究者选择的挽救性化疗相比,纳武利尤单抗使1年总生存中位数提高了2.2倍(36.0%对16.6%)。向成功方案——帕博利珠单抗联合铂类和静脉输注氟尿嘧啶的转变,在作为R/M HNSCC的一线治疗时,其总生存期(中位数,13.6个月对10.1个月)超过了过去基于西妥昔单抗的铂类和氟尿嘧啶联合治疗的金标准。然而,许多患者对PD-1/PD-L1检查点抑制剂治疗仍无反应,这表明对免疫疗法存在先天性、适应性或快速获得性耐药。本文综述聚焦于HNSCC背景下针对PD-1/PD-L1信号通路的ICI耐药机制。在过去5年里,人们对肿瘤细胞中检查点抑制耐药的潜在机制有了更深入的了解,例如:肿瘤细胞通过I类人类白细胞抗原(HLA)使抗原呈递机制功能失调来实现适应,细胞周期中重新引入细胞周期蛋白D-细胞周期蛋白依赖性激酶(CDK)4复合物,富集CD44+癌症干细胞样细胞,或IKZF1基因发生失活突变;通过干扰素-γ调节基因的突变、干扰素基因刺激物(STING)通路的抑制或由遗传性营养性缺铁状态导致T细胞功能和增殖受损;癌细胞通过代谢物如GTP环化水解酶1、四氢生物蝶呤、犬尿氨酸、吲哚胺2,3-双加氧酶和精氨酸酶1的变化进行代谢重编程;树突状细胞缺陷、CD-69充足状态;以及包括淋巴细胞激活基因-3(LAG3)、T细胞免疫球蛋白和ITIM结构域(TIGIT)/CD155通路、T细胞免疫球蛋白粘蛋白-3(TIM-3)和含V结构域的T细胞激活抑制性Ig(VISTA)在内的替代免疫检查点上调或激活。本文还讨论了几种可能预测对PD-1/PD-L1检查点免疫疗法反应或耐药的潜在生物标志物或生物特征。