Bücklein Veit, Limmroth Christina, Kampmann Eric, Schuebbe Gesa, Issels Rolf, Roeder Falk, Angele Martin, Dürr Hans Roland, Knösel Thomas, Abdel-Rahman Sultan, Di Gioia Dorit, Lindner Lars H
Department of Medicine III, University Hospital, LMU Munich, Munich, Germany.
Medizinische Klinik Köln-Holweide, Cologne, Germany.
Sarcoma. 2020 Feb 27;2020:6901678. doi: 10.1155/2020/6901678. eCollection 2020.
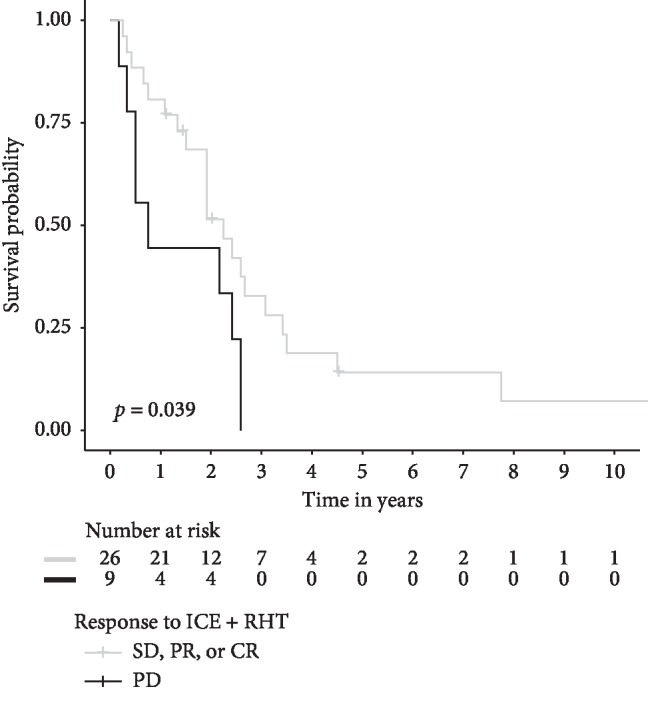
Patients with localized relapse of soft-tissue sarcoma (STS) after anthracycline-based chemotherapy have a dismal prognosis, particularly when surgery is not possible. To facilitate resection and improve long-term tumor control, we applied an intensified perioperative treatment consisting of ICE (ifosfamide 6 g/m, carboplatin 400 mg/m, and etoposide 600 mg/m) in combination with regional hyperthermia (RHT) to maximize local control. Here, we retrospectively evaluate the safety and efficacy of this strategy. Patients aged ≥18 years with locally advanced high-risk STS, either with or without metastasis, treated with ICE + RHT after the failure of first-line anthracycline-based chemotherapy were included in this analysis. Radiographic response, toxicity, progression-free survival (PFS), and overall survival (OS) were assessed. Between 1996 and 2018, 213 sarcoma patients received ICE at our centre. Of these, 110 patients met the selection criteria (progressive disease, suitable high-grade STS histology, anthracycline pretreatment, RHT treatment) for this analysis. Fifty-four patients had locally advanced disease without metastases (LA-STS), and 56 patients had additional metastatic disease (M-STS). Disease control was achieved in 59% of LA-STS patients and in 47% of M-STS patients. For LA-STS, 21% of the patients achieved radiographic response, facilitating resection in 4 patients (7%), compared with 11% of the M-STS patients, facilitating resection in 5 patients (9%). PFS was significantly longer in LA-STS than in M-STS (10 vs. 4 months, < 0.0001). Median OS was 26 months in LA-STS and 12 months in M-STS. Disease control was the only independent prognostic factor for improved OS in multivariate analysis. Toxicity was high with neutropenic fever occurring in 25% of the patients and three therapy-related deaths (3%). ICE + RHT demonstrated activity in high-risk STS and facilitated resection in selected patients after anthracycline failure. Disease control was associated with improved OS. Based on the observed toxicities, the dose should be reduced to 75%.
接受过蒽环类药物化疗后出现软组织肉瘤(STS)局部复发的患者预后不佳,尤其是无法进行手术时。为了便于切除并改善长期肿瘤控制,我们采用了一种强化围手术期治疗方案,即ICE(异环磷酰胺6 g/m²、卡铂400 mg/m²和依托泊苷600 mg/m²)联合区域热疗(RHT),以最大限度地实现局部控制。在此,我们回顾性评估了该策略的安全性和有效性。本分析纳入了年龄≥18岁、一线蒽环类药物化疗失败后接受ICE + RHT治疗的局部晚期高危STS患者,无论有无转移。评估了影像学反应、毒性、无进展生存期(PFS)和总生存期(OS)。1996年至2018年期间,213例肉瘤患者在我们中心接受了ICE治疗。其中,110例患者符合本分析的选择标准(疾病进展、合适的高级别STS组织学、蒽环类药物预处理、RHT治疗)。54例患者为无转移的局部晚期疾病(LA-STS),56例患者有额外的转移性疾病(M-STS)。59%的LA-STS患者和47%的M-STS患者实现了疾病控制。对于LA-STS,21%的患者实现了影像学反应,4例患者(7%)因此便于进行切除,而M-STS患者为11%,5例患者(9%)便于进行切除。LA-STS患者的PFS显著长于M-STS患者(10个月对4个月,P < 0.0001)。LA-STS患者的中位OS为26个月,M-STS患者为12个月。在多变量分析中,疾病控制是OS改善的唯一独立预后因素。毒性较高,25%的患者发生中性粒细胞减少性发热,3例患者(3%)死于治疗相关原因。ICE + RHT在高危STS中显示出活性,并在蒽环类药物治疗失败后的部分患者中便于进行切除。疾病控制与OS改善相关。基于观察到的毒性,剂量应减至75%。