Department of Neurology, Faculty of Medicine, Albert Szent-Györgyi Clinical Center, University of Szeged, Semmelweis u. 6, 6725, Szeged, Hungary.
Department of Pathology, Faculty of Medicine, Albert Szent-Györgyi Clinical Center, University of Szeged, Állomás u. 2, 6725, Szeged, Hungary.
J Neural Transm (Vienna). 2020 Jun;127(6):963-972. doi: 10.1007/s00702-020-02174-2. Epub 2020 Mar 19.
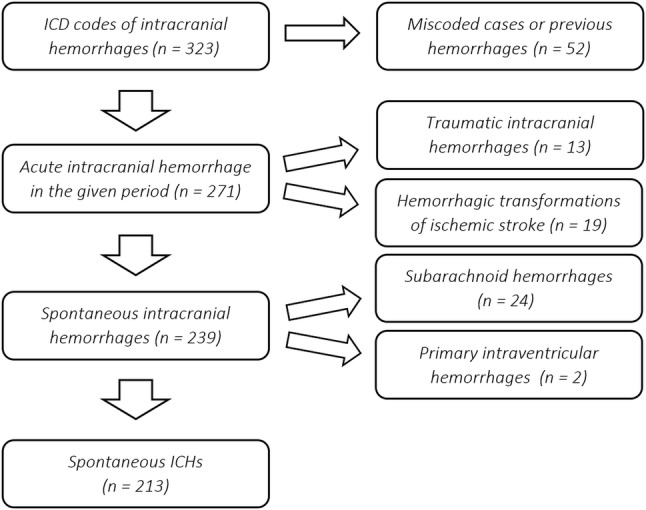
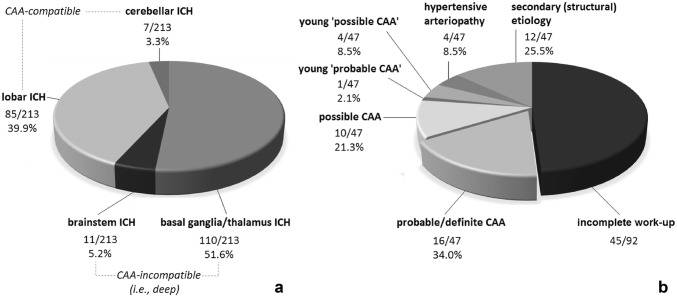
Despite its clinical relevance, cerebral amyloid angiopathy (CAA) is underdiagnosed worldwide. This retrospective study aimed to assess the incidence, etiology, predictors, and outcome of intracerebral hemorrhages (ICHs) in this region, with special focus on possible underlying CAA. Database screening of acute cares with intracranial hemorrhage diagnosis within 01/07/2014-01/07/2018 were conducted analyzing medical records and imaging. Spontaneous ICHs were classified as deep (basal ganglionic/thalamic/brainstem) and lobar/cerebellar (i.e., CAA-compatible) ICHs. Probable/definite CAA was established using the modified Boston criteria in a subgroup with 'complete' radiological/neuropathological work-up. The ability of several factors to discriminate between deep and lobar/cerebellar ICHs, between probable/definite CAA and non-probable CAA cases, and to predict 1-month case fatality was assessed. Of the 213 ICHs identified, 121 were in deep and 92 in lobar/cerebellar localization. Sub-analysis of 47 lobar/cerebellar ICHs with 'complete' work-up identified 16 probable/definite CAA patients, yielding an estimated 14.7% prevalence of CAA-related ICHs. Chronic hypertension was the most prevalent risk factor for all types of ICHs (including CAA-related), with hypertensive excess and younger age being independent predictors of deep whereas antiplatelet use of lobar/cerebellar localization. The 1-month case fatality was 33.8%, driven predominantly by age and INR > 1.4. Probable/definite CAA diagnosis was independently predicted by age, prior intracranial hemorrhage, and antiplatelet use. First in this region and among the few in the literature, this study reports a remarkable prevalence of CAA-related ICHs, emphasizing the need for an increased awareness of CAA and its therapeutic implications, especially regarding antiplatelets among the elderly.
尽管脑淀粉样血管病(CAA)具有临床相关性,但在全球范围内的诊断率仍然较低。本回顾性研究旨在评估该地区颅内出血(ICH)的发生率、病因、预测因素和转归,特别关注可能潜在的 CAA。通过对 2014 年 7 月 1 日至 2018 年 7 月 1 日期间在急性护理中诊断为颅内出血的患者进行数据库筛选,分析病历和影像学资料。自发性 ICH 分为深部(基底节/丘脑/脑干)和脑叶/小脑(即 CAA 型)ICH。在亚组中,通过改良波士顿标准来确定可能/明确的 CAA,该亚组进行了“完整”的影像学/神经病理学检查。评估了几个因素区分深部和脑叶/小脑 ICH、区分可能/明确 CAA 和非可能 CAA 病例以及预测 1 个月病死率的能力。在确定的 213 例 ICH 中,121 例位于深部,92 例位于脑叶/小脑。对 47 例进行“完整”检查的脑叶/小脑 ICH 的亚组分析确定了 16 例可能/明确的 CAA 患者,估计 CAA 相关 ICH 的患病率为 14.7%。慢性高血压是所有类型 ICH(包括 CAA 相关 ICH)最常见的危险因素,高血压过度和年龄较轻是深部 ICH 的独立预测因素,而抗血小板治疗则是脑叶/小脑 ICH 的独立预测因素。1 个月病死率为 33.8%,主要由年龄和 INR>1.4 驱动。可能/明确的 CAA 诊断与年龄、既往颅内出血和抗血小板使用独立相关。这是该地区首次报告,也是文献中少数报告之一,该研究报告了 CAA 相关 ICH 的显著患病率,强调需要提高对 CAA 的认识及其治疗意义,特别是在老年人中对抗血小板治疗的认识。