Paolillo Emily W, Pasipanodya Elizabeth C, Moore Raeanne C, Pence Brian W, Atkinson Joseph Hampton, Grelotti David J, Grant Igor, Heaton Robert K, Moore David J
San Diego State University, UC San Diego Joint Doctoral Program in Clinical Psychology, San Diego, CA.
Department of Psychiatry, UC San Diego, San Diego, CA.
J Acquir Immune Defic Syndr. 2020 Jul 1;84(3):304-312. doi: 10.1097/QAI.0000000000002346.
Higher cumulative burden of depression among people with HIV (PWH) is associated with poorer health outcomes; however, longitudinal relationships with neurocognition are unclear. This study examined hypotheses that among PWH, (1) higher cumulative burden of depression would relate to steeper declines in neurocognition, and (2) visit-to-visit depression severity would relate to fluctuations in neurocognition within persons.
Data were collected at a university-based research center from 2002 to 2016.
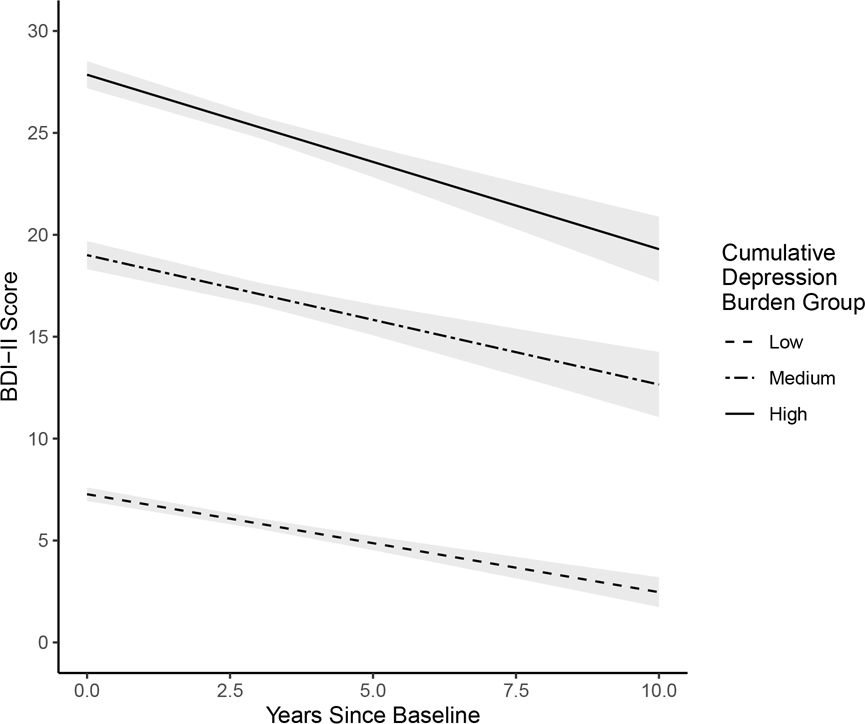
Participants included 448 PWH followed longitudinally. All participants had >1 visit (M = 4.97; SD = 3.53) capturing depression severity (Beck Depression Inventory-II) and neurocognition (comprehensive test battery). Cumulative burden of depression was calculated using an established method that derives weighted depression severity scores by time between visits and total time on study. Participants were categorized into low (67%), medium (15%), and high (18%) depression burden. Multilevel modeling examined between- and within-person associations between cumulative depression burden and neurocognition over time.
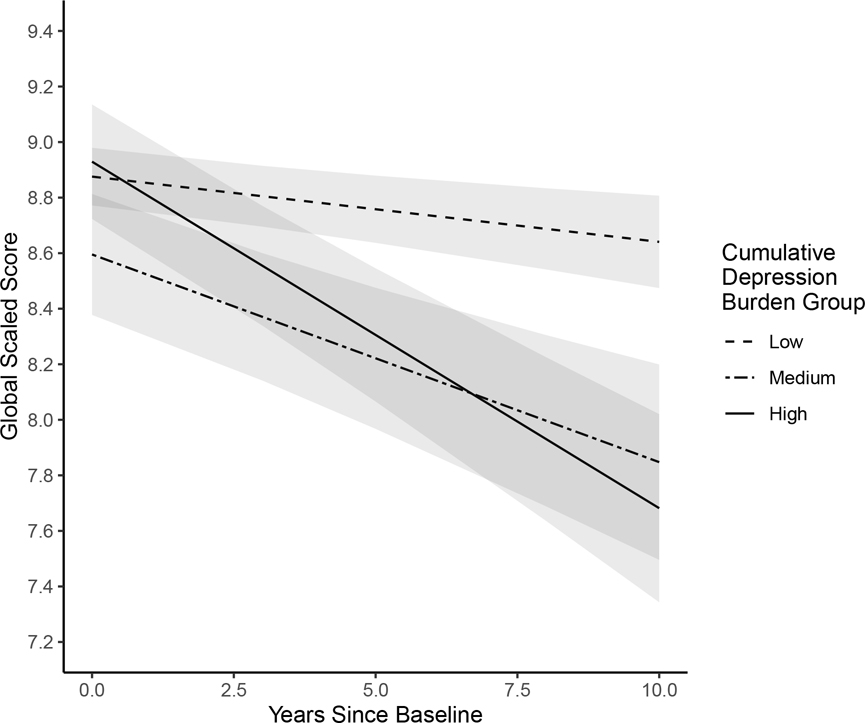
The high depression burden group demonstrated steeper global neurocognitive decline compared with the low depression burden group (b = -0.100, P = 0.001); this was driven by declines in executive functioning, delayed recall, and verbal fluency. Within-person results showed that compared with visits when participants reported minimal depressive symptoms, their neurocognition was worse when they reported mild (b = -0.12, P = 0.04) or moderate-to-severe (b = -0.15, P = 0.03) symptoms; this was driven by worsened motor skills and processing speed.
High cumulative burden of depression is associated with worsening neurocognition among PWH, which may relate to poor HIV-related treatment outcomes. Intensive interventions among severely depressed PWH may benefit physical, mental, and cognitive health.
艾滋病毒感染者(PWH)中抑郁症的累积负担较高与较差的健康结果相关;然而,与神经认知的纵向关系尚不清楚。本研究检验了以下假设:在PWH中,(1)较高的抑郁症累积负担与神经认知的更急剧下降有关,(2)每次就诊时的抑郁严重程度与个体内部神经认知的波动有关。
2002年至2016年在一个大学研究中心收集数据。
参与者包括448名接受纵向随访的PWH。所有参与者都有超过1次就诊(M = 4.97;SD = 3.53),记录抑郁严重程度(贝克抑郁量表第二版)和神经认知(综合测试组)。使用一种既定方法计算抑郁症的累积负担,该方法通过就诊间隔时间和研究总时间得出加权抑郁严重程度分数。参与者被分为低(67%)、中(15%)和高(18%)抑郁负担组。多水平模型研究了累积抑郁负担与神经认知随时间的组间和个体内部关联。
与低抑郁负担组相比,高抑郁负担组的整体神经认知下降更急剧(b = -0.100,P = 0.001);这是由执行功能、延迟回忆和语言流畅性的下降驱动的。个体内部结果显示,与参与者报告极少抑郁症状的就诊相比,当他们报告轻度(b = -0.12,P = 0.04)或中度至重度(b = -0.15,P = 0.03)症状时,他们的神经认知更差;这是由运动技能和处理速度恶化驱动的。
抑郁症的高累积负担与PWH的神经认知恶化有关,这可能与艾滋病毒相关治疗结果不佳有关。对严重抑郁的PWH进行强化干预可能有益于身体、心理和认知健康。