Cleveland Clinic Florida, Weston, FL, USA.
University of Cincinnati Medical Center, Cincinnati, OH, USA
Eur Respir Rev. 2020 Mar 20;29(155). doi: 10.1183/16000617.0146-2019. Print 2020 Mar 31.
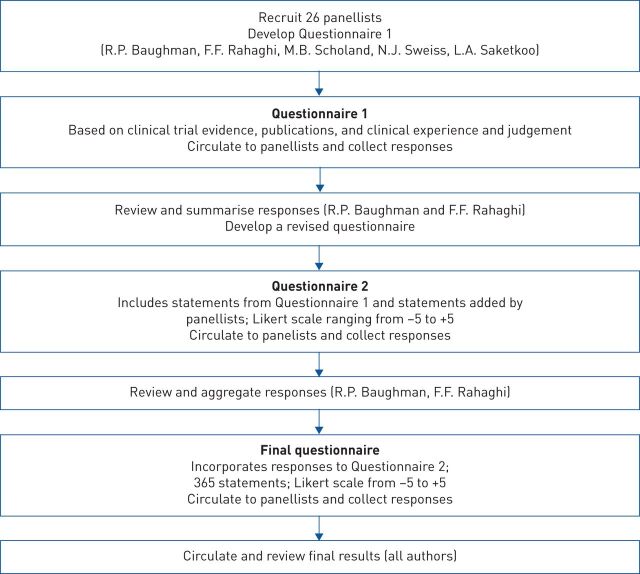
Pulmonary sarcoidosis presents substantial management challenges, with limited evidence on effective therapies and phenotypes. In the absence of definitive evidence, expert consensus can supply clinically useful guidance in medicine. An international panel of 26 experts participated in a Delphi process to identify consensus on pharmacological management in sarcoidosis with the development of preliminary recommendations.The modified Delphi process used three rounds. The first round focused on qualitative data collection with open-ended questions to ensure comprehensive inclusion of expert concepts. Rounds 2 and 3 applied quantitative assessments using an 11-point Likert scale to identify consensus.Key consensus points included glucocorticoids as initial therapy for most patients, with non-biologics (immunomodulators), usually methotrexate, considered in severe or extrapulmonary disease requiring prolonged treatment, or as a steroid-sparing intervention in cases with high risk of steroid toxicity. Biologic therapies might be considered as additive therapy if non-biologics are insufficiently effective or are not tolerated with initial biologic therapy, usually with a tumour necrosis factor-α inhibitor, typically infliximab.The Delphi methodology provided a platform to gain potentially valuable insight and interim guidance while awaiting evidenced-based contributions.
肺结节病的治疗存在诸多挑战,针对有效的治疗方法和疾病表型的证据有限。在缺乏明确证据的情况下,专家共识可为医学提供具有临床应用价值的指导。一个由 26 名国际专家组成的小组参与了德尔菲法流程,以确定结节病药物治疗的共识,并制定初步建议。该改良德尔菲法共使用了三轮。第一轮采用开放式问题进行定性数据收集,以确保全面纳入专家的观点。第二轮和第三轮采用 11 点李克特量表进行定量评估,以确定共识。关键的共识要点包括大多数患者初始治疗使用糖皮质激素,在需要长期治疗的严重或肺外疾病或有发生糖皮质激素毒性高风险的情况下,使用非生物制剂(免疫调节剂),通常是甲氨蝶呤;在非生物制剂治疗效果不佳或不能耐受时,可作为初始生物制剂治疗的附加治疗,通常使用肿瘤坏死因子-α抑制剂,如英夫利昔单抗。德尔菲法为获得潜在有价值的见解和临时指导提供了一个平台,同时等待基于证据的贡献。