Momenipur Amirmasoud, Pennathur Priyadarshini R
Information and Cognitive Systems Engineering Research Laboratory, Department of Industrial and Systems Engineering, University of Iowa, Iowa City, IA 52242, USA.
Int J Ind Ergon. 2019 Jul;72:338-346. doi: 10.1016/j.ergon.2019.06.012. Epub 2019 Jul 1.
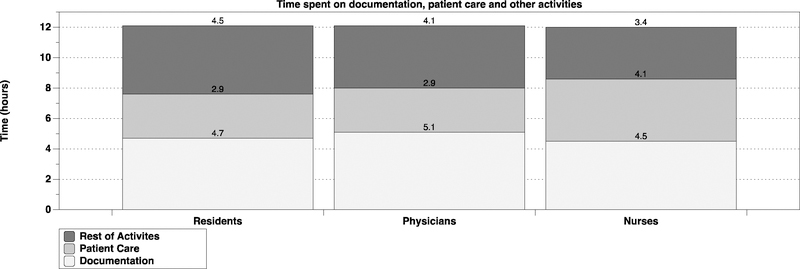
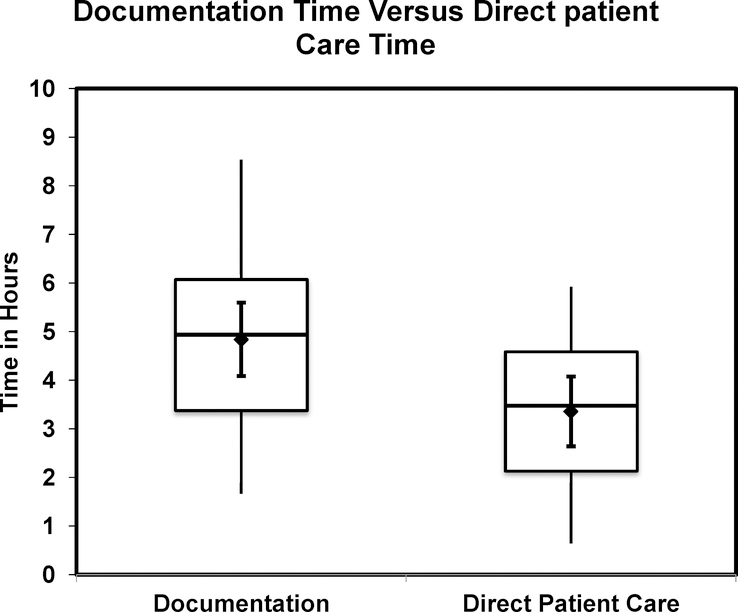
US hospitals now fully embrace electronic documentation systems as a way to reduce medical errors and improve patient safety outcomes. Whether spending time on electronic documentation detracts from the time available for direct patient care, however, is still unresolved. There is no knowledge on the permanent effects of documenting electronically and whether it takes away significant time from patient care when the healthcare information system is mature. To understand the time spent on documentation, direct patient care tasks, and other clinical tasks in a mature information system, we conducted an observational and interview study in a midwestern academic hospital. The hospital implemented an electronic medical record system 11 years ago. We observed 22 health care workers across intensive care units, inpatient floors, and an outpatient clinic in the hospital. Results show that healthcare workers spend more time on documentation activities compared to patient care activities. Clinical roles have no influence on the time spent on documentation. This paper describes results on the time spent between documentation and patient care tasks, and discusses implications for future practice.
The study applies to healthcare industry that faces immense challenges in balancing documentation activities and patient care activities.
美国医院现在完全采用电子文档系统作为减少医疗差错和改善患者安全结果的一种方式。然而,花时间在电子文档上是否会减少可用于直接患者护理的时间,这一点仍未得到解决。对于电子记录的长期影响以及当医疗信息系统成熟时它是否会从患者护理中占用大量时间,我们还一无所知。为了了解在一个成熟的信息系统中花在文档记录、直接患者护理任务和其他临床任务上的时间,我们在一家中西部学术医院进行了一项观察性和访谈研究。该医院11年前实施了电子病历系统。我们观察了医院重症监护病房、住院楼层和门诊诊所的22名医护人员。结果表明,与患者护理活动相比,医护人员在文档记录活动上花费的时间更多。临床角色对文档记录所花费的时间没有影响。本文描述了文档记录和患者护理任务之间所花费时间的结果,并讨论了对未来实践的影响。
该研究适用于在平衡文档记录活动和患者护理活动方面面临巨大挑战的医疗行业。