Department of Health Promotion, Norwegian Institute of Public Health, Bergen, Norway.
Department of Clinical Science, University of Bergen, Bergen, Norway.
Int J Health Policy Manag. 2020 Mar 1;9(3):96-107. doi: 10.15171/ijhpm.2019.84.
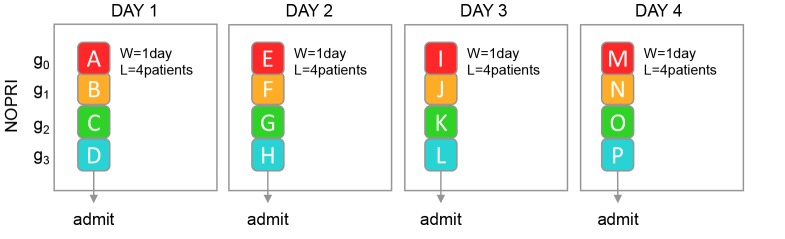
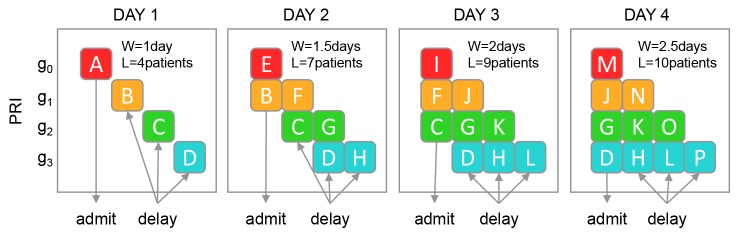
Policies assigning low-priority patients treatment delays for care, in order to make room for patients of higher priority arriving later, are common in secondary healthcare services today. Alternatively, each new patient could be granted the first available appointment. We aimed to investigate whether prioritisation can be part of the reason why waiting times for care are often long, and to describe how departments can improve their waiting situation by changing away from prioritisation.
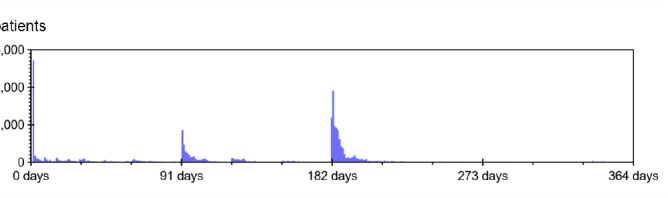
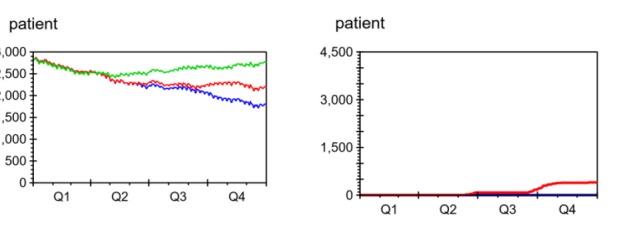
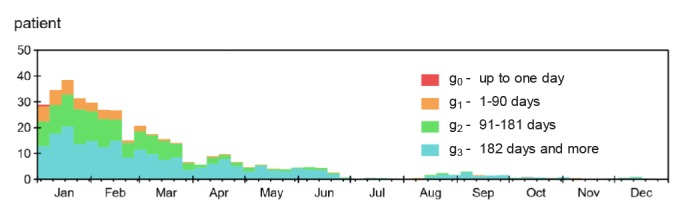
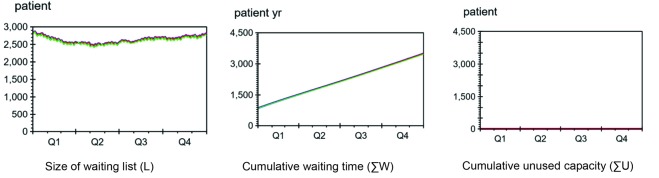
We used patient flow data from 2015 at the Department of Otorhinolaryngology, Haukeland University Hospital, Norway. In Dynaplan Smia, Dynaplan AS, dynamic simulations were used to compare how waiting time, size and shape of the waiting list, and capacity utilisation developed with and without prioritisation. Simulations were started from the actual waiting list at the beginning of 2015, and from an empty waiting list (simulating a new department with no initial patient backlog).
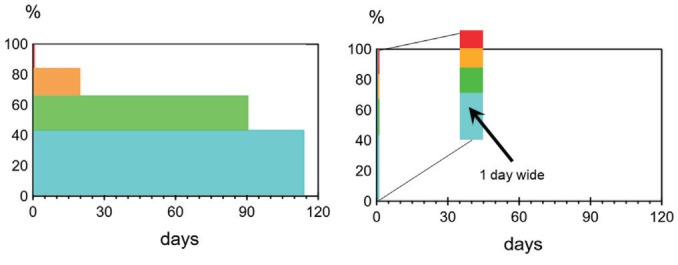
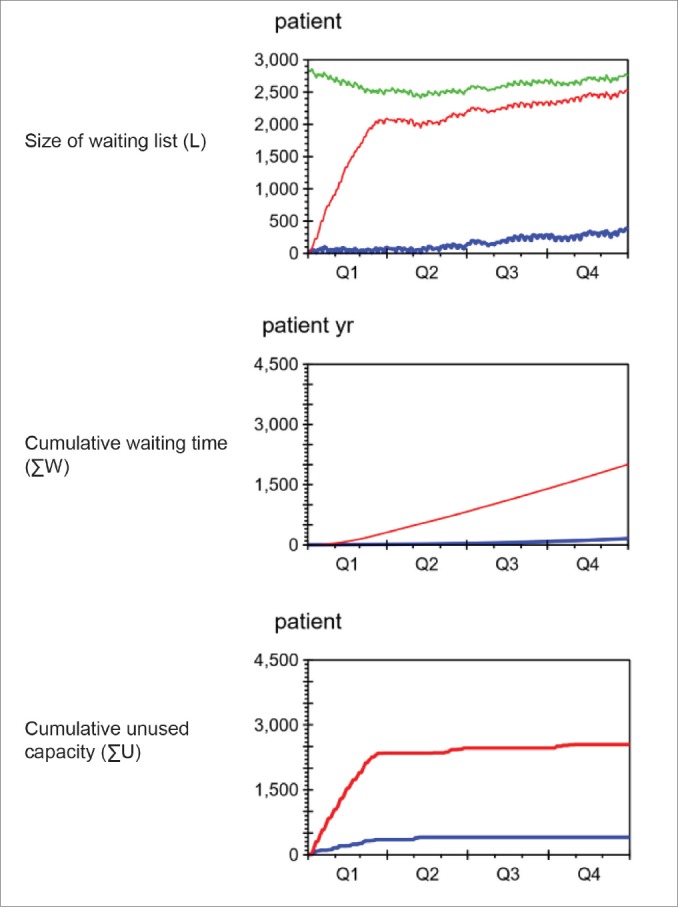
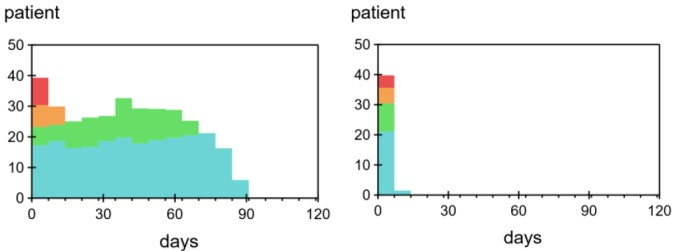
From an empty waiting list and with capacity equal to demand, waiting times were built 7 times longer when prioritising than when not. Prioritisation also led to poor resource utilisation and short-lived effects of extra capacity. Departments where prioritisation is causing long waits can improve their situation by temporarily bringing capacity above demand and introducing "first come, first served" instead of prioritisation.
A poor appointment allocation policy can build long waiting times, even when capacity is sufficient to meet demand. By bringing waiting times down and going away from prioritisation, the waiting list size and average waiting times at the studied department could be maintained almost 90% below the current level - without requiring permanent change in the capacity/demand ratio.
为了给后来的高优先级患者腾出空间,将低优先级患者的治疗延迟安排的政策在二级医疗服务中很常见。或者,每个新患者都可以获得第一个可用的预约。我们旨在调查优先级是否是导致护理等待时间通常较长的原因之一,并描述部门如何通过放弃优先级来改善其等待情况。
我们使用了来自挪威豪克兰大学医院耳鼻喉科 2015 年的患者流量数据。在 Dynaplan Smia 和 Dynaplan AS 中,使用动态模拟来比较有无优先级的情况下等待时间、等待列表的大小和形状以及容量利用率的发展情况。模拟从 2015 年初的实际等待列表开始,并从空的等待列表(模拟一个没有初始患者积压的新部门)开始。
从空的等待列表开始,并且容量等于需求,当进行优先级排序时,等待时间比不进行优先级排序时长 7 倍。优先级排序还导致资源利用率差和额外容量的短暂效果。对于因优先级排序而导致长时间等待的部门,可以通过暂时将容量提高到需求以上并引入“先来先服务”而不是优先级排序来改善其情况。
即使容量足以满足需求,较差的预约分配政策也会导致长时间的等待。通过降低等待时间并放弃优先级排序,可以将研究部门的等待列表大小和平均等待时间维持在当前水平的近 90%以下 - 而无需永久改变容量/需求比例。