Department of Radiation Oncology, University Hospital of Muenster, Muenster, Germany.
Department of Medicine A (Hematology, Oncology, and Pneumology), University Hospital of Muenster, Muenster, Germany.
Oncologist. 2020 May;25(5):e816-e832. doi: 10.1634/theoncologist.2019-0783. Epub 2020 Mar 27.
This article reports on the long-term impact of radiotherapy adapted to stage, histology, and previous resection in a large cohort of patients with intestinal lymphoma (iL) treated with definitive or adjuvant curative-intent radiation therapy (RT) ± chemotherapy (CHOP, MCP, or COP).
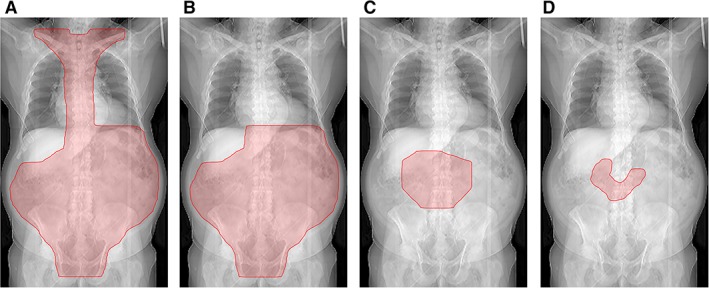
In two consecutive prospective study designs, 134 patients with indolent (stage IE-IIE) or aggressive (stage IE-IVE) iL were referred to 61 radiotherapeutic institutions between 1992 and 2003. Patients with indolent iL received extended field (EF) 30 Gy (+10 Gy boost in definitive treatment); patients with aggressive iL received involved field (IF) (EF) 40 Gy by means of stage-, histology-, and operation-adapted radiation fields.
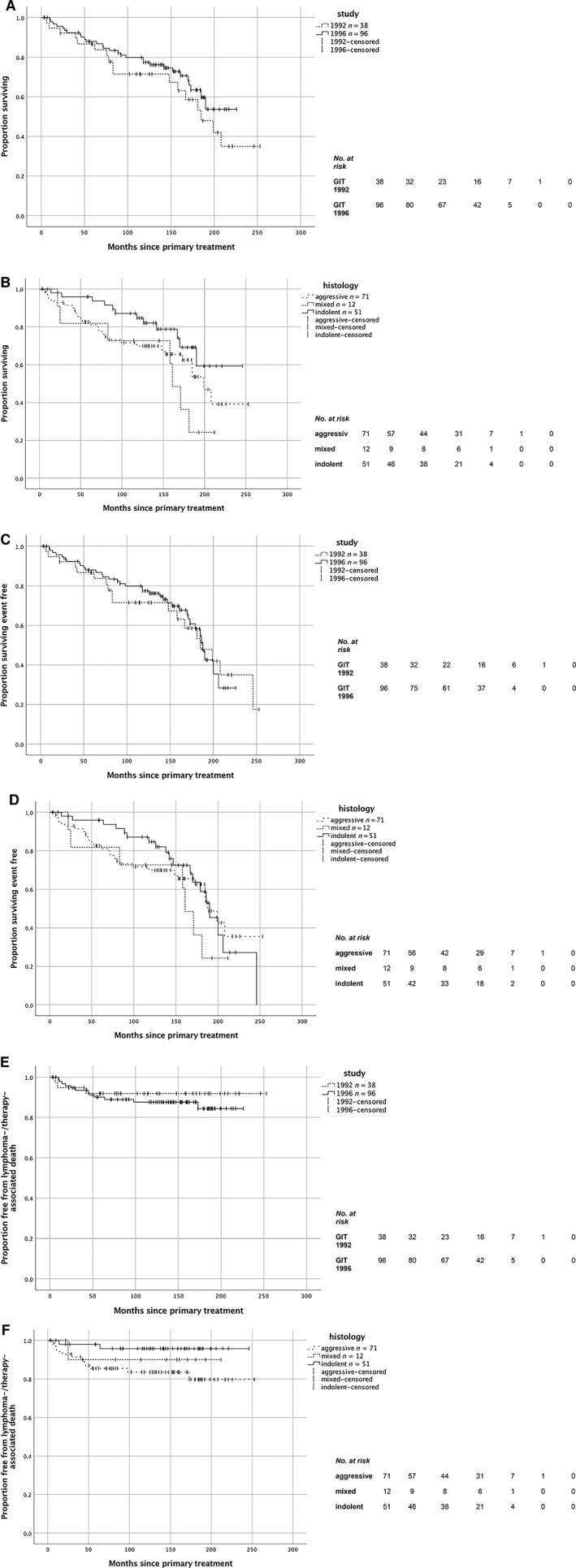
The patients had median age 58 years and were predominantly male (2:1). Histology showed aggressive prevalence (1.6:1), stage IE-to-stage IIE ratio of iL 1.04:1, and localized stages-to-advanced stages ratio of aggressive lymphoma 23:1. Median follow-up was in total 11.7 years: 10.0 years in the first study, GIT (GastroIntestinal-Tract) 1992, and 11.8 years in the second study, GIT 1996. Lymphoma involvement was predominantly a single intestinal lesion (82.1%). Decrease of radiation field size from EF to IF in stage I aggressive iL from GIT 1992 to GIT 1996 resulted in a nonsignificant partial reduction of chronic toxicity while maintaining comparable survival rates (5-year overall survival 87.9 vs. 86.7%, 10-year overall survival 77.4 vs. 71.5%) with nonsignificant difference in event-free survival (5-year event-free survival 82.6 vs. 86.7%, 10-year event-free survival 69.7 vs. 71.5%) and lymphoma-specific survival (5-year lymphoma-specific survival 90.1 vs. 91.9%, 10-year lymphoma-specific survival 87.6% vs. 91.9%). Comparative dose calculation of two still available indolent duodenal lymphoma computed tomography scans revealed lower radiation exposure to normal tissues from applying current standard involved site RT (ISRT) 30 Gy in both cases.
RT adapted to stage, histology, and resection in multimodal treatment of iL, despite partially decreasing field size (EF to IF), achieves excellent local tumor control and survival rates. The use of modern RT technique and target volume with ISRT offers the option of further reduction of normal tissue complication probability.
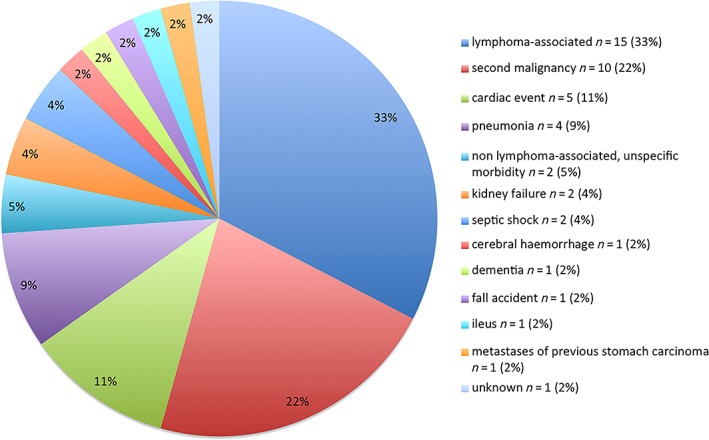
Although patients with intestinal lymphoma (iL) are heterogeneous according to histology and subtype, they benefit from radiotherapy. Prospective study data from 134 patients with indolent iL (stage IE-IIE) or aggressive iL (stage IE-IVE) show 100% tumor control after definitive or adjuvant curative-intent radiation therapy ± chemotherapy. Radiation treatment was applied between 1992 and 2003. Median follow-up in total was 11.7 years. No radiotherapy-associated death occurred. Relapse developed in 15.7% of the entire cohort; distant failure was more frequent than local (4:1). Normal tissue complication probability can be further improved using modern involved site radiation therapy techniques.
本文报道了在接受根治性或辅助性意向放疗(RT)±化疗(CHOP、MCP 或 COP)治疗的大量肠淋巴瘤(iL)患者中,根据分期、组织学和既往切除情况调整放疗的长期影响。
在两个连续的前瞻性研究设计中,134 例惰性(IE-IIE 期)或侵袭性(IE-IVE 期)iL 患者于 1992 年至 2003 年期间被转诊至 61 个放射治疗机构。惰性 iL 患者接受扩展野(EF)30Gy(在根治性治疗中加 10Gy 推量);侵袭性 iL 患者接受基于分期、组织学和手术的受累野(IF)(EF)40Gy。
患者的中位年龄为 58 岁,以男性为主(2:1)。组织学显示侵袭性为主(1.6:1),IE 期至 IIE 期 iL 的比例为 1.04:1,局限性侵袭性淋巴瘤的比例为 23:1。中位随访时间为 11.7 年:第一研究中为 10.0 年(GIT,1992 年),第二研究中为 11.8 年(GIT,1996 年)。淋巴瘤受累主要为单个肠道病变(82.1%)。1992 年至 1996 年,从 EF 到 IF 减少侵袭性 I 期 iL 的放疗野大小,导致慢性毒性的部分降低,但保持了可比的生存率(5 年总生存率 87.9% vs. 86.7%,10 年总生存率 77.4% vs. 71.5%),无事件生存率(5 年无事件生存率 82.6% vs. 86.7%,10 年无事件生存率 69.7% vs. 71.5%)和淋巴瘤特异性生存率(5 年淋巴瘤特异性生存率 90.1% vs. 91.9%,10 年淋巴瘤特异性生存率 87.6% vs. 91.9%)无显著差异。对仍有的两个惰性十二指肠淋巴瘤 CT 扫描进行比较剂量计算,发现目前采用标准受累部位放疗(ISRT)30Gy 时,正常组织的放射暴露量较低。
尽管 iL 患者根据组织学和亚型存在异质性,但多模式治疗中根据分期、组织学和切除情况进行的 RT 仍能获得良好的局部肿瘤控制和生存率。现代 RT 技术和 ISRT 靶区的应用为进一步降低正常组织并发症概率提供了可能。
尽管肠淋巴瘤(iL)患者在组织学和亚型上存在异质性,但他们受益于放疗。134 例惰性 iL(IE-IIE 期)或侵袭性 iL(IE-IVE 期)患者的前瞻性研究数据显示,在接受根治性或辅助性意向放疗(RT)±化疗后,100%的肿瘤得到控制。放疗于 1992 年至 2003 年期间进行。总中位随访时间为 11.7 年。无放疗相关死亡发生。整个队列中有 15.7%的患者出现复发;远处失败比局部更常见(4:1)。使用现代受累部位放疗技术可进一步提高正常组织并发症概率。