Ishii Daizo, Nakagawa Daichi, Zanaty Mario, Roa Jorge A, Al Kasab Sami, Shaban Amir, Hudson Joseph S, Osorno-Cruz Carlos, Byer Stefano, Allan Lauren, Torner James C, Awad Issam A, Carroll Timothy J, Samaniego Edgar A, Hasan David M
Department of Neurosurgery, University of Iowa Hospitals and Clinics, Iowa City, IA 52242, USA.
Department of Neurosurgery, University of Tokyo, Tokyo 113 8654, Japan.
J Clin Med. 2020 Apr 1;9(4):979. doi: 10.3390/jcm9040979.
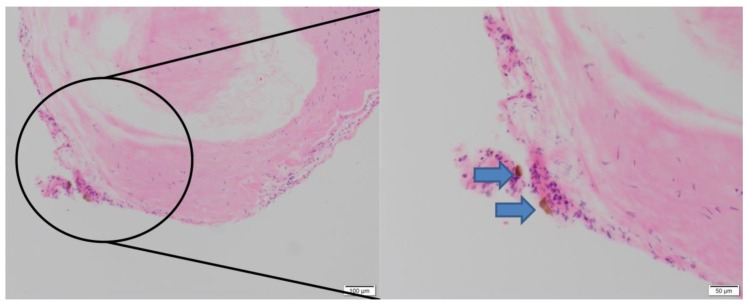
MR-quantitative susceptibility mapping (QSM) can identify microbleeds (MBs) in intracranial aneurysm (IA) wall associated with sentinel headache (SH) preceding subarachnoid hemorrhage. However, its use is limited, due to associated skull base bonny and air artifact. MR-vessel wall imaging (VWI) is not limited by such artifact and therefore could be an alternative to QSM. The purpose of this study was to investigate the correlation between QSM and VWI in detecting MBs and to help develop a diagnostic strategy for SH.
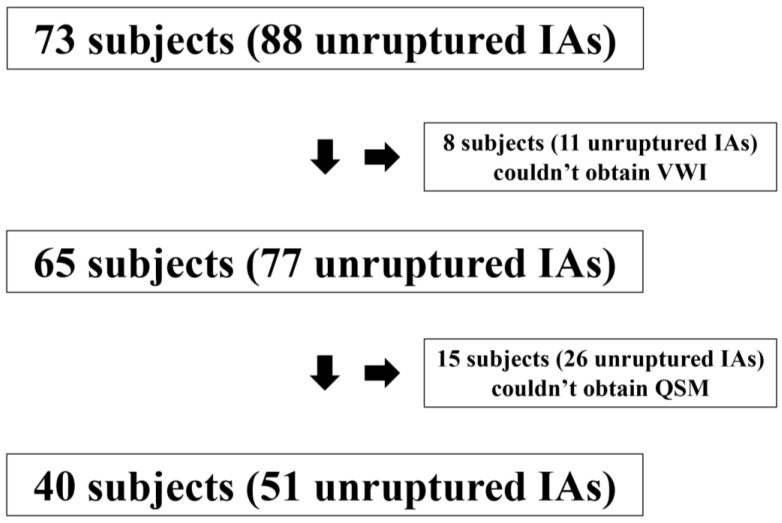
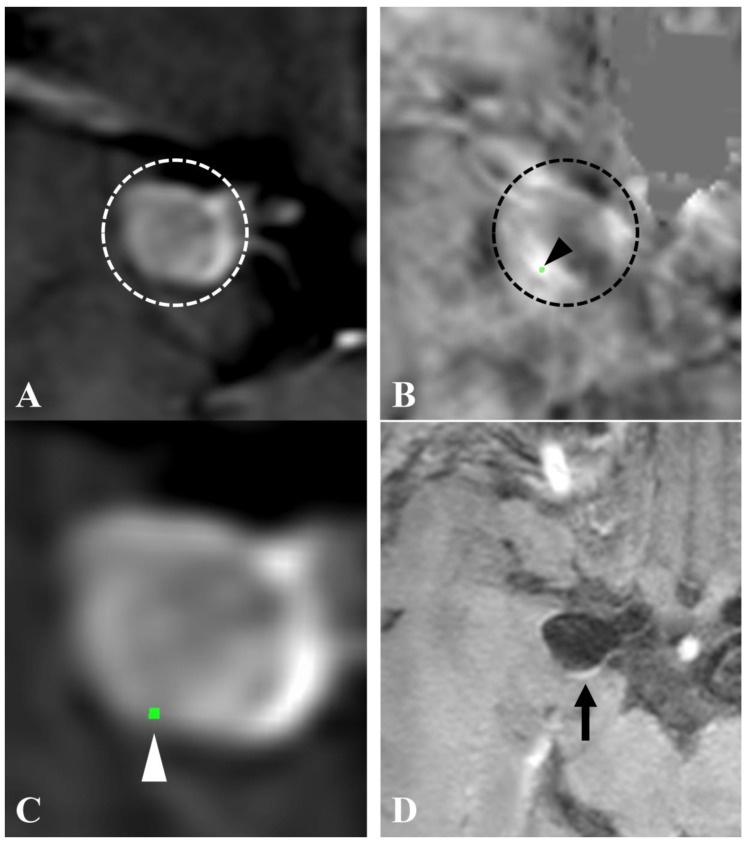
We performed a prospective study of subjects with one or more unruptured IAs in our hospital. All subjects underwent evaluation using 3T-MRI for MR angiography (MRA), QSM, and pre- and post-contrast VWI of the IAs. Presence/absence of MBs detected by QSM was correlated with aneurysm wall enhancement (AWE) on VWI.
A total of 40 subjects harboring 51 unruptured IAs were enrolled in the study. MBs evident on the QSM sequence was detected in 12 (23.5%) IAs of 11 subjects. All these subjects had a history of severe headache suggestive of SH. AWE was detected in 22 (43.1%) IAs. Using positive QSM as a surrogate for MBs, the sensitivity, specificity, positive predictive value, and negative predictive value of AWE on VWI for detecting MBs were 91.7%, 71.8%, 50%, and 96.6%, respectively.
Positive QSM findings strongly suggested the presence of MBs with SH, whereas, the lack of AWE on VWI can rule it out with a probability of 96.6%. If proven in a larger cohort, combining QSM and VWI could be an adjunctive tool to help diagnose SH, especially in cases with negative or non-diagnostic CT and lumbar puncture.
磁共振定量磁化率成像(QSM)能够识别颅内动脉瘤(IA)壁内与蛛网膜下腔出血前的哨兵头痛(SH)相关的微出血(MBs)。然而,由于存在颅底骨质和空气伪影,其应用受到限制。磁共振血管壁成像(VWI)不受此类伪影的限制,因此可能是QSM的替代方法。本研究的目的是探讨QSM与VWI在检测MBs方面的相关性,并帮助制定SH的诊断策略。
我们对我院有一个或多个未破裂IA的受试者进行了一项前瞻性研究。所有受试者均接受3T-MRI检查,以进行磁共振血管造影(MRA)、QSM以及IA的对比剂增强前后VWI检查。QSM检测到的MBs的有无与VWI上的动脉瘤壁强化(AWE)相关。
本研究共纳入了40例患有51个未破裂IA的受试者。在11例受试者的12个(23.5%)IA中检测到QSM序列上明显的MBs。所有这些受试者都有提示SH的严重头痛病史。在22个(43.1%)IA中检测到AWE。以阳性QSM作为MBs的替代指标,VWI上AWE检测MBs的敏感性、特异性、阳性预测值和阴性预测值分别为91.7%、71.8%、50%和96.6%。
QSM阳性结果强烈提示存在伴有SH的MBs,而VWI上缺乏AWE则可在96.6%的概率上排除。如果在更大的队列中得到证实,联合使用QSM和VWI可能是一种辅助工具,有助于诊断SH,尤其是在CT和腰椎穿刺结果为阴性或无法诊断的情况下。