Dept. of Otorhinolaryngology/Head and Neck Surgery, University Medical Center Groningen, University of Groningen, Groningen, The Netherlands.
Dept. of Pathology and Medical Biology, University Medical Center Groningen, University of Groningen, Groningen, The Netherlands.
Clin Otolaryngol. 2020 Jul;45(4):486-494. doi: 10.1111/coa.13540. Epub 2020 Apr 23.
The choice of treatment in laryngeal cancer is mainly based on tumor stage, post-treatment morbidity and quality of life. Biological tumor markers might also be of potential clinical relevance.
The aim was to systematically review the value of published biological tumor markers to predict local control in laryngeal cancer patients treated with definitive radiotherapy.
Systematic review.
PubMed, Embase, Cochrane Library.
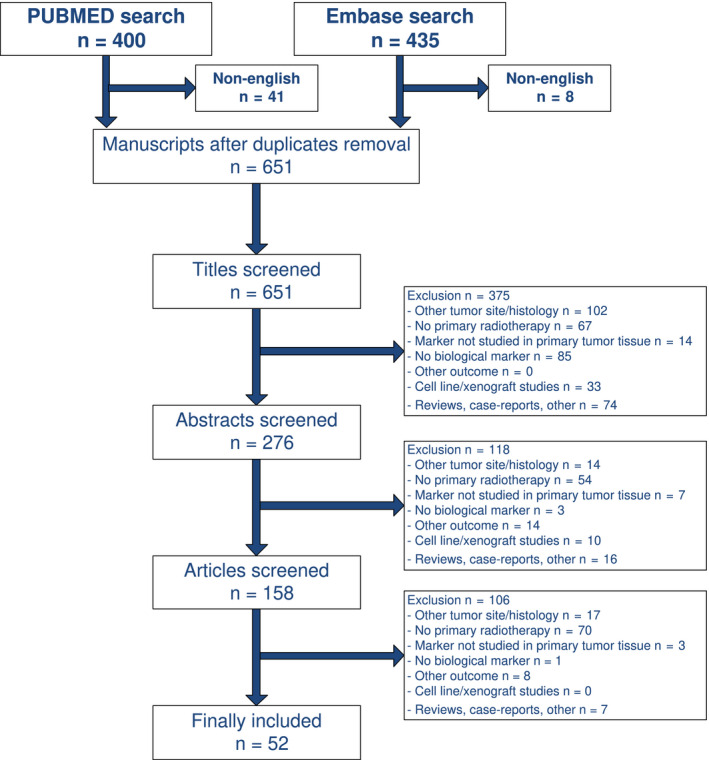
A literature search was performed using multiple terms for laryngeal cancer, radiotherapy, biological markers, detection methods and local control or survival. Studies regarding the relation between biological tumor markers and local control or survival in laryngeal cancer patients primarily treated with radiotherapy were included. Markers were clustered on biological function. Quality of all studies was assessed. Study selection, data extraction and quality assessment was performed by two independent reviewers.
A total of 52 studies out of 618 manuscripts, concerning 118 markers, were included. EGFR and P53 showed consistent evidence for not being predictive of local control after primary radiotherapy, whereas proliferation markers (ie high Ki-67 expression) showed some, but no consistent, evidence for being predictive of better local control. Other clusters of markers (markers involved in angiogenesis and hypoxia, apoptosis markers, cell cycle, COX-2 and DNA characteristics) showed no consistent evidence towards being predictors of local control after primary radiotherapy.
Cell proliferation could be of potential interest for predicting local control after primary radiotherapy in laryngeal cancer patients, whereas EGFR and p53 are not predictive in contrast to some previous analyses. Large diversity in research methods is found between studies, which results in contradictory outcomes. Future studies need to be more standardised and well described according to the REMARK criteria in order to have better insight into which biomarkers can be used as predictors of local control after primary radiotherapy.
喉癌的治疗选择主要基于肿瘤分期、治疗后发病率和生活质量。生物肿瘤标志物也可能具有潜在的临床相关性。
系统评价已发表的生物肿瘤标志物预测接受根治性放疗的喉癌患者局部控制的价值。
系统评价。
PubMed、Embase、Cochrane 图书馆。
使用多个术语对喉癌、放疗、生物标志物、检测方法和局部控制或生存进行了文献检索。纳入了主要接受放疗治疗的喉癌患者生物标志物与局部控制或生存之间关系的研究。根据生物功能对标志物进行聚类。评估所有研究的质量。由两名独立评审员进行研究选择、数据提取和质量评估。
从 618 篇手稿中总共选出 52 篇研究,涉及 118 个标志物。EGFR 和 P53 一致表明不能预测原发性放疗后的局部控制,而增殖标志物(即高 Ki-67 表达)则显示出一些但不一致的证据,表明能更好地预测局部控制。其他标志物簇(涉及血管生成和缺氧的标志物、凋亡标志物、细胞周期、COX-2 和 DNA 特征)没有一致的证据表明能预测原发性放疗后的局部控制。
细胞增殖可能对预测喉癌患者接受原发性放疗后的局部控制具有潜在意义,而与之前的一些分析相反,EGFR 和 p53 则不具有预测性。研究之间研究方法的多样性很大,导致结果相互矛盾。未来的研究需要更加标准化和详细描述,以根据 REMARK 标准更好地了解哪些生物标志物可用作原发性放疗后局部控制的预测因子。