Nkieri Matthieu, Mbo Florent, Kavunga Papy, Nganzobo Pathou, Mafolo Titus, Selego Chalet, Mwamba Miaka Eric
Bagata Health Zone, Avenue Kalanganda N 10, Mwendo Bagata,32 Kwilu Province, Democratic Republic of the Congo.
National Sleeping Sickness Control Program (PNLTHA) (PNMLS building), Boulevard Triomphale Crossing Av. 24 November, 10 Kinshasa, Democratic Republic of the Congo.
Trop Med Infect Dis. 2020 Apr 4;5(2):53. doi: 10.3390/tropicalmed5020053.
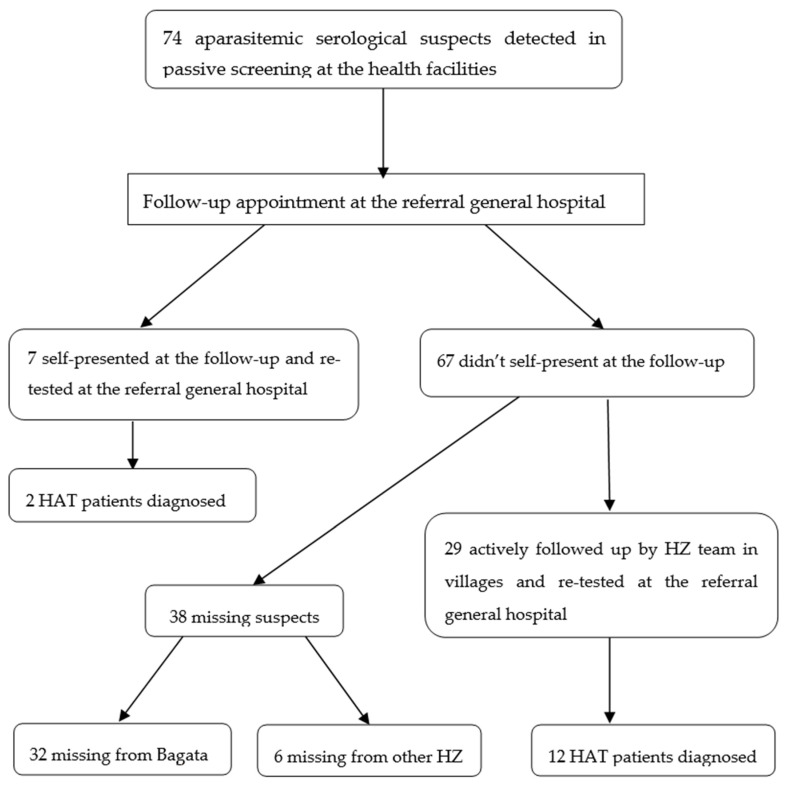
The World Health Organization aims for the elimination of Human African Trypanosomiasis (HAT) as a public health problem by 2020 and for full elimination (absence of new cases) by 2030. One of strategies to achieve this is the active follow-up of all HAT serological suspects found during passive screening who have never been re-tested for parasitology. This is important because these cases can maintain HAT transmission and may be responsible for reemergence of the disease. In order to improve case finding at low cost in the targeted population, a general recall was transmitted to aparasitemic serological suspects about the availability of confirmation services at the general referral hospital. Transport was facilitated for re-testing. The initial examinations were carried out in Health Centers from Bagata Health Zone (HZ) in the Democratic Republic of the Congo between January 2017 and April 2019. This strategy of using a HZ team has not been previously documented. From a total sample of 74 serological suspects listed by the health centers, 36 cases were re-examined at the general reference hospital; 19% (7/36) self-presented and 81% (29/36) were actively followed up by HZ personnel. Of those re-examined at the general reference hospital, 39% (14/36) resulted in a parasitologically confirmed case. Of the 14 people diagnosed with HAT, 14% (2/14) self-presented and the remaining 86% (12/14) were diagnosed in suspects who were actively followed up. This new strategy of facilitating transport from the villages added value by contributing to the detection of 12 HAT cases, compared to the passive approach, waiting for self-reference, which resulted in the detection of 2 new HAT cases. The cost per detected patient was 70 USD from the group of 7 suspects who self-presented for testing at the hospital and 346 USD per detected case for the group of 29 patients who were actively followed up by health zone staff. Targeted active follow-up of aparasitemic serological suspects by HZ teams is a cost-effective and promising approach to identifying additional cases of HAT in areas of very low prevalence, which would contribute to the HAT elimination goal set by the World Health Organization.
世界卫生组织的目标是到2020年将人类非洲锥虫病(HAT)作为一个公共卫生问题予以消除,并到2030年实现完全消除(无新病例)。实现这一目标的策略之一是对在被动筛查期间发现的所有从未接受过寄生虫学复查的HAT血清学疑似病例进行积极随访。这一点很重要,因为这些病例可能维持HAT的传播,并可能导致该疾病再次出现。为了以低成本在目标人群中改善病例发现情况,向寄生虫血症血清学疑似病例发出了一份关于综合转诊医院可提供确诊服务的一般性召回通知。为复查提供了交通便利。2017年1月至2019年4月期间,在刚果民主共和国巴加塔卫生区(HZ)的卫生中心进行了初步检查。此前尚未记录过使用卫生区团队的这一策略。在卫生中心列出的74例血清学疑似病例的总样本中,有36例在综合参考医院接受了复查;其中19%(7/36)是自行前来的,81%(29/36)是由卫生区工作人员积极随访的。在综合参考医院接受复查的病例中,39%(14/36)经寄生虫学确诊。在被诊断为HAT的14人中,14%(2/14)是自行前来的,其余86%(12/14)是在被积极随访的疑似病例中确诊的。与被动方法(等待自行前来)相比,这种促进从村庄前来就医的新策略有助于发现12例HAT病例,而被动方法仅发现了2例新的HAT病例。自行到医院检测的7名疑似病例组中,每发现一例患者的成本为70美元,而卫生区工作人员积极随访的29名患者组中,每发现一例病例的成本为346美元。卫生区团队对寄生虫血症血清学疑似病例进行有针对性的积极随访,是在极低流行率地区发现更多HAT病例的一种具有成本效益且前景光明的方法,这将有助于实现世界卫生组织设定的消除HAT目标。