Frazer Lauren C, O'Connell Amy E
Division of Newborn Medicine, Boston Children's Hospital, Boston, MA, USA.
Department of Pediatrics, Harvard Medical School, Boston, MA, USA.
Pediatr Res. 2021 Feb;89(3):549-553. doi: 10.1038/s41390-020-0886-6. Epub 2020 Apr 8.
Prematurity presents a diagnostic challenge in interpreting primary immunodeficiency (PID) testing.
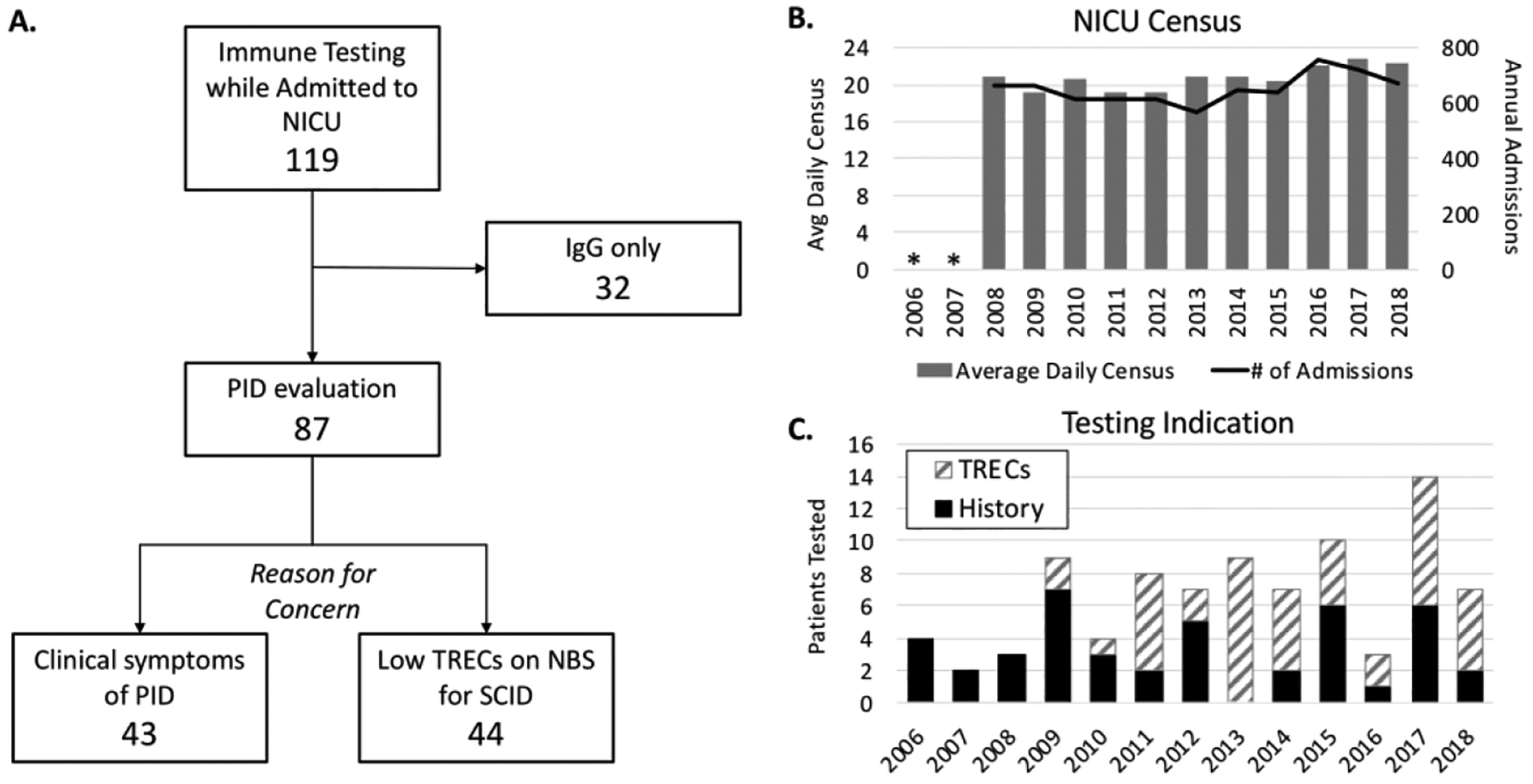
We retrospectively reviewed the charts of all infants in our level IV referral neonatal intensive care unit (NICU) in Massachusetts, with immunologic testing performed from 2006 to 2018.
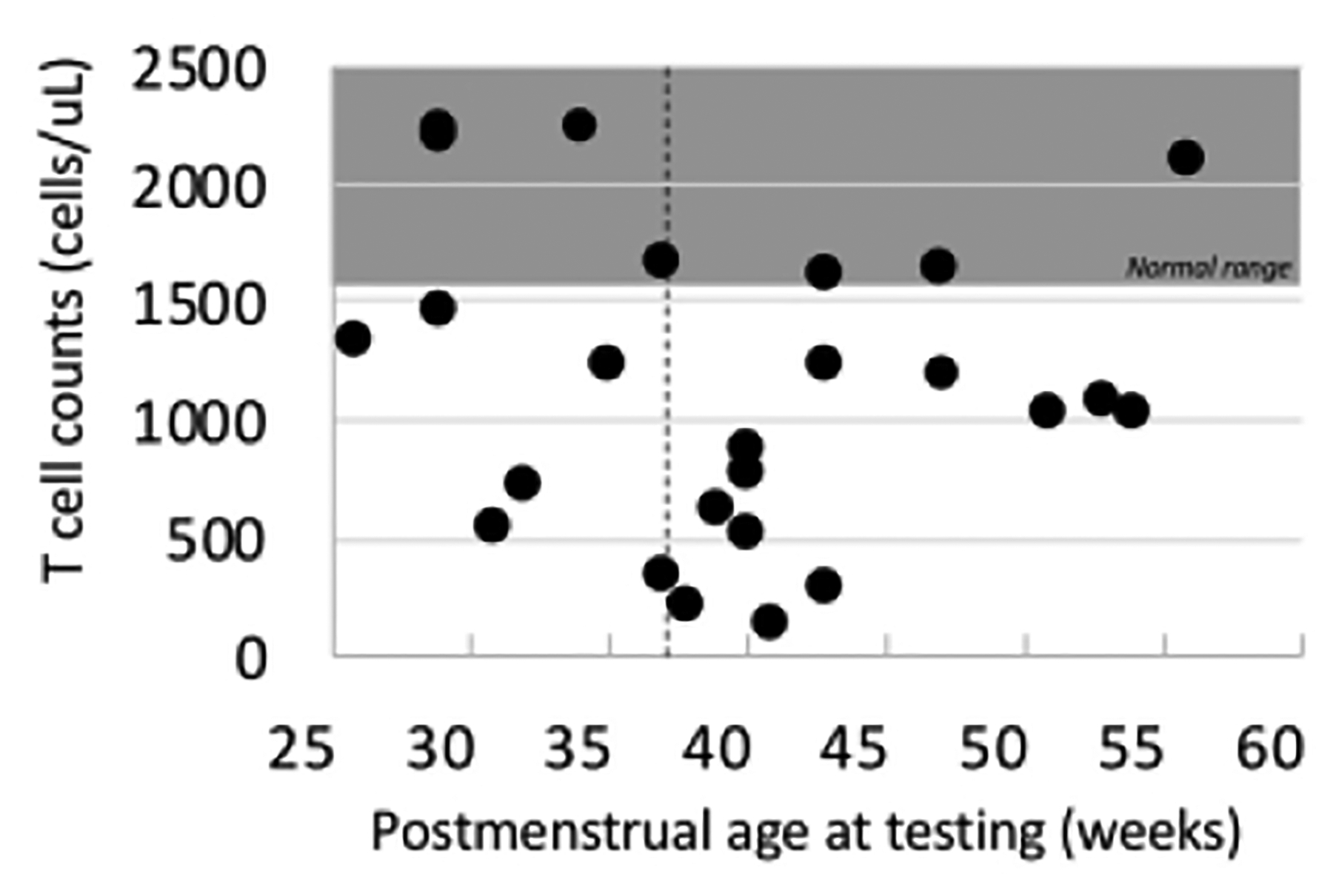
The overall rate of PID testing was enriched in our population, with 1% of admitted patients having extended immunologic testing. The addition of TREC (T cell receptor excision circle) newborn screening in Massachusetts in 2009 increased the proportion of infants tested for PID in our NICU by 3-fold (1.21% post-newborn screening (NBS) vs. 0.46% pre-NBS). A majority of the term and late preterm (≥34 weeks) infants (31 of 41, 76%), as well as very premature (29-33 weeks) infants (12 of 17, 71%), who had immune testing, had a genetic diagnosis associated with secondary immunodeficiency or a PID. Most infants who were born extremely premature (EP, <29 weeks) (25 of 29, 86%) had no identifiable cause of immunodeficiency besides prematurity, despite a mean postmenstrual age of 40.1 weeks at the time of testing.
Persistent immune derangements were present within a subgroup of the EP population through term postmenstrual age. EP infants with significant infectious history and abnormal immune testing at term-corrected age should be considered for genetic testing.
The role of immunologic testing in the premature population is unclear, we therefore reviewed the records of all infants in our NICU who had immunologic testing, to rule out immunodeficiency, done from 2006 to 2018. The addition of newborn screening for SCID in 2009 doubled the number of infants who had immune investigations. The extremely premature cohort included many infants with persistent immune derangements through term-corrected gestational age, suggesting a persistent effect of prematurity on immune development and potential function. We propose that former premature infants with clinical evidence of immunodeficiency and sustained immune abnormalities by term-corrected age undergo genetic testing for immunodeficiency.
早产在解释原发性免疫缺陷(PID)检测结果时带来诊断挑战。
我们回顾性分析了马萨诸塞州四级转诊新生儿重症监护病房(NICU)2006年至2018年期间所有接受免疫检测的婴儿病历。
我们研究人群中PID检测的总体比例较高,1%的入院患者接受了全面免疫检测。2009年马萨诸塞州增加了TREC(T细胞受体切除环)新生儿筛查,使我们NICU中接受PID检测的婴儿比例增加了3倍(新生儿筛查后为1.21%,筛查前为0.46%)。大多数足月儿和晚期早产儿(≥34周)(41例中的31例,76%)以及极早产儿(29 - 33周)(17例中的12例,71%)在接受免疫检测后,得到了与继发性免疫缺陷或PID相关的基因诊断。大多数极早产儿(EP,<29周)(29例中的25例,86%)除早产外没有可识别的免疫缺陷原因,尽管检测时平均月经后年龄为40.1周。
在极早产人群的一个亚组中,直至足月月经后年龄仍存在持续的免疫紊乱。对于有显著感染史且在足月校正年龄时免疫检测异常的极早产婴儿,应考虑进行基因检测。
免疫检测在早产人群中的作用尚不清楚,因此我们回顾了2006年至2018年期间我们NICU中所有接受免疫检测以排除免疫缺陷的婴儿记录。2009年增加的严重联合免疫缺陷(SCID)新生儿筛查使接受免疫检查的婴儿数量增加了一倍。极早产队列包括许多在足月校正胎龄时存在持续免疫紊乱的婴儿,提示早产对免疫发育和潜在功能有持续影响。我们建议,对于有免疫缺陷临床证据且在足月校正年龄时持续存在免疫异常的 former 早产儿,应进行免疫缺陷基因检测。 (注:原文中“former”在这里表意不明,可能是“former premature infants”表述有误,译者按原文翻译)