Department of Anaesthesia, National University Hospital, Singapore; Yong Loo Lin School of Medicine, National University of Singapore, Singapore.
Department of Anaesthesia, National University Hospital, Singapore; Yong Loo Lin School of Medicine, National University of Singapore, Singapore.
Am J Obstet Gynecol. 2020 Jul;223(1):66-74.e3. doi: 10.1016/j.ajog.2020.04.005. Epub 2020 Apr 10.
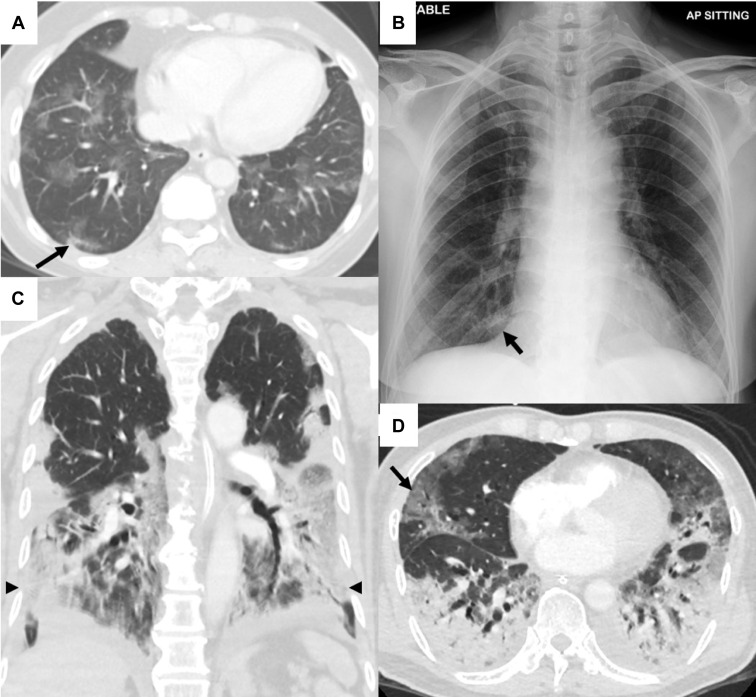
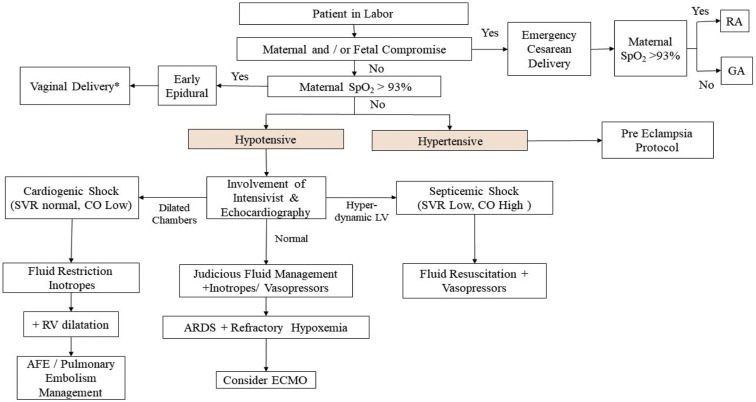
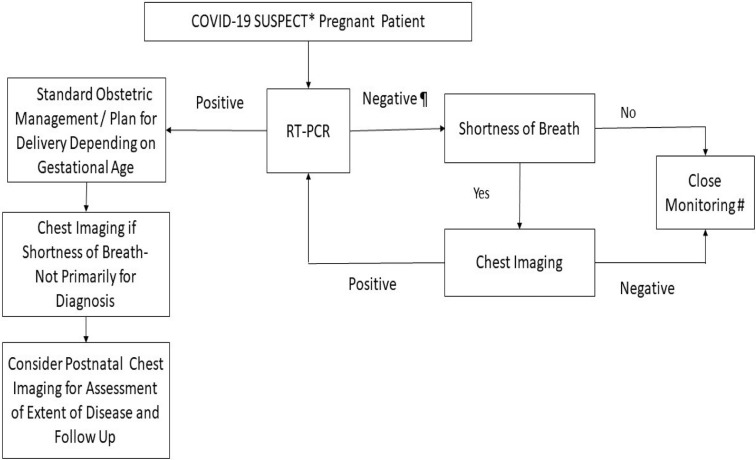
Coronavirus disease 2019, caused by the severe acute respiratory syndrome coronavirus 2, has been declared a pandemic by the World Health Organization. As the pandemic evolves rapidly, there are data emerging to suggest that pregnant women diagnosed as having coronavirus disease 2019 can have severe morbidities (up to 9%). This is in contrast to earlier data that showed good maternal and neonatal outcomes. Clinical manifestations of coronavirus disease 2019 include features of acute respiratory illnesses. Typical radiologic findings consists of patchy infiltrates on chest radiograph and ground glass opacities on computed tomography scan of the chest. Patients who are pregnant may present with atypical features such as the absence of fever as well as leukocytosis. Confirmation of coronavirus disease 2019 is by reverse transcriptase-polymerized chain reaction from upper airway swabs. When the reverse transcriptase-polymerized chain reaction test result is negative in suspect cases, chest imaging should be considered. A pregnant woman with coronavirus disease 2019 is at the greatest risk when she is in labor, especially if she is acutely ill. We present an algorithm of care for the acutely ill parturient and guidelines for the protection of the healthcare team who is caring for the patient. Key decisions are made based on the presence of maternal and/or fetal compromise, adequacy of maternal oxygenation (SpO >93%) and stability of maternal blood pressure. Although vertical transmission is unlikely, there must be measures in place to prevent neonatal infections. Routine birth processes such as delayed cord clamping and skin-to-skin bonding between mother and newborn need to be revised. Considerations can be made to allow the use of screened donated breast milk from mothers who are free of coronavirus disease 2019. We present management strategies derived from best available evidence to provide guidance in caring for the high-risk and acutely ill parturient. These include protection of the healthcare workers caring for the coronavirus disease 2019 gravida, establishing a diagnosis in symptomatic cases, deciding between reverse transcriptase-polymerized chain reaction and chest imaging, and management of the unwell parturient.
新型冠状病毒病 2019,由严重急性呼吸系统综合症冠状病毒 2 引起,已被世界卫生组织宣布为大流行。随着大流行的迅速发展,有数据表明,被诊断患有新型冠状病毒病 2019 的孕妇可能会出现严重的并发症(高达 9%)。这与早期数据显示的良好母婴结局形成了鲜明对比。新型冠状病毒病 2019 的临床表现包括急性呼吸道疾病的特征。典型的放射学表现为胸片上的斑片状浸润和胸部计算机断层扫描上的磨玻璃样混浊。孕妇可能表现出不典型的特征,如无发热和白细胞增多。新型冠状病毒病 2019 的确诊是通过上呼吸道拭子的逆转录聚合酶链反应。在疑似病例中,当逆转录聚合酶链反应检测结果为阴性时,应考虑进行胸部成像。患有新型冠状病毒病 2019 的孕妇在分娩时风险最大,尤其是当她病情严重时。我们提出了一种针对急性发病产妇的护理算法,并为照顾患者的医疗保健团队制定了保护指南。关键决策是基于母婴和/或胎儿是否受损、母体氧合是否充足(SpO2 >93%)以及母体血压是否稳定。虽然垂直传播不太可能,但必须采取措施预防新生儿感染。需要修改常规分娩过程,如延迟脐带夹闭和母婴皮肤接触。可以考虑允许使用来自未感染新型冠状病毒病 2019 的母亲的筛查捐赠母乳。我们提出了基于最佳现有证据的管理策略,为照顾高危和急性发病的产妇提供指导。这些策略包括保护照顾新型冠状病毒病 2019 孕妇的医护人员,在有症状的病例中做出诊断,在逆转录聚合酶链反应和胸部成像之间做出选择,以及对不适产妇进行管理。