The State Key Laboratory of Respiratory Diseases, Guangzhou Institute of Respiratory Health, The First Affiliated Hospital of Guangzhou Medical University, 151 Yanjiang Street West, Guangzhou, 510120, Guangdong, China.
Respir Res. 2020 Apr 15;21(1):85. doi: 10.1186/s12931-020-01355-7.
Intraoperative Extracorporeal membrane oxygenation (ECMO) is increasingly being applied as life-support for lung transplantation patients. However, factors associated with this procedure in lung transplantation patients have not yet been characterized. The aim of this study was to identify preoperative factors of intraoperative ECMO support during lung transplantation and to evaluated the outcome of lung transplantation patients supported with ECMO.
Patients underwent lung transplantation treated with and without ECMO in Guangzhou Institute of Respiratory Diseases between January 2015 to August 2018 were retrospectively reviewed. Patient demographics and clinical variables were collected and analyzed. Multivariate logistic regression was performed to identify factors independently associated with intraoperative extracorporeal membrane oxygenation support during lung transplantation.
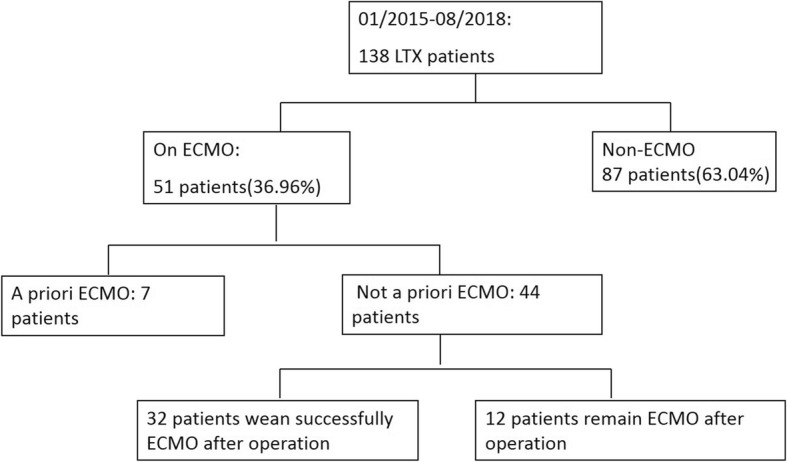
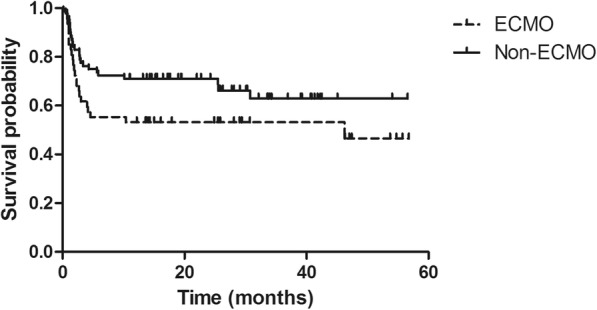
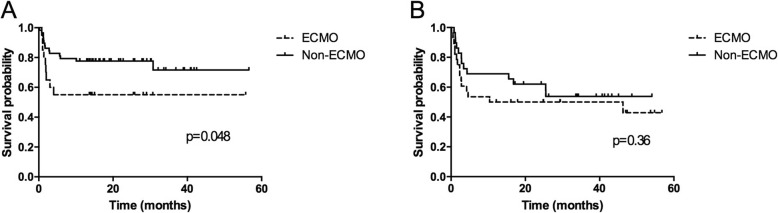
During the study period, 138 patients underwent lung transplantation at our institution, the mean LAS was (56.63 ± 18.39) (range, 32.79 to 88.70). Fourty four patients were treated with veno-venous/veno-arterial ECMO. Among the patients, 32 patients wean successfully ECMO after operation, 12 patients remain ECMO after operation, and 32 patients (62.74%) survived to hospital discharge. In multiple analysis, the following factors were associated with intraoperative ECMO support: advanced age, high PAP before operation, duration of mechanical ventilation before operation, a higher APACHE II and primary diagnosis for transplantation. The overall survival rates at 1, 3, and 12 months were 90.91, 72.73, and 56.81% in the ECMO group, and 95.40, 82.76, and 73.56% in the non-ECMO group, respectively (log-rank P = 0.081). Patients who underwent single lung transplant had a lower survival rates in ECMO group as compared with non-ECMO group at 1, 3, and 12 months (90.47% vs 98.25, 71.43% vs 84.21, and 52.38% vs 75.44%) (log-rank P = 0.048).
The preoperative factors of intraoperative ECMO support during lung transplantation included age, high PAP before operation, preoperative mechanical ventilation, a higher APACHE II and primary diagnosis for transplantation based on multivariate analysis.
体外膜肺氧合(ECMO)在肺移植患者中作为生命支持越来越多地应用。然而,肺移植患者中与该手术相关的因素尚未明确。本研究旨在确定肺移植术中 ECMO 支持的术前因素,并评估 ECMO 支持的肺移植患者的预后。
回顾性分析 2015 年 1 月至 2018 年 8 月在广州呼吸疾病研究所接受肺移植治疗且接受和未接受 ECMO 的患者。收集并分析患者的人口统计学和临床变量。采用多变量逻辑回归分析确定与肺移植术中 ECMO 支持独立相关的因素。
在研究期间,我院共有 138 例患者接受了肺移植,平均 LAS 为(56.63±18.39)(范围 32.79 至 88.70)。44 例患者接受了静脉-静脉/静脉-动脉 ECMO 治疗。在这些患者中,32 例患者术后成功撤离 ECMO,12 例患者术后仍在使用 ECMO,32 例患者(62.74%)存活至出院。多因素分析显示,以下因素与术中 ECMO 支持相关:高龄、术前 PAP 升高、术前机械通气时间延长、APACHE II 评分升高和移植的主要诊断。ECMO 组的 1、3 和 12 个月的总体生存率分别为 90.91%、72.73%和 56.81%,非 ECMO 组分别为 95.40%、82.76%和 73.56%(log-rank P=0.081)。在 ECMO 组中,与非 ECMO 组相比,接受单肺移植的患者在 1、3 和 12 个月时的生存率较低(90.47%比 98.25%,71.43%比 84.21%,52.38%比 75.44%)(log-rank P=0.048)。
基于多因素分析,肺移植术中 ECMO 支持的术前因素包括年龄、术前 PAP 升高、术前机械通气、APACHE II 评分升高和移植的主要诊断。