Department of Neurology and Institute of Health Science, Gyeongsang National University College of Medicine, Jinju, South Korea.
Department of Neurology, Mayo Clinic, 5777 East Mayo Boulevard, Phoenix, AZ, 85054, USA.
J Headache Pain. 2020 Apr 15;21(1):33. doi: 10.1186/s10194-020-01103-8.
Close associations between insomnia with other clinical factors have been identified in migraine, but there have been few studies investigating associations between insomnia and clinical factors in patients with persistent post-traumatic headache (PPTH). The study objective was to contrast the severity of insomnia symptoms in PPTH, migraine, and healthy controls, and to identify factors associated with insomnia in patients with PPTH vs. migraine.
In this cross-sectional cohort study, 57 individuals with PPTH attributed to mild traumatic brain injury, 39 with migraine, and 39 healthy controls were included. Participants completed a detailed headache characteristics questionnaire, the Migraine Disability Assessment Scale (MIDAS), Insomnia Severity Index (ISI), Hyperacusis Questionnaire (HQ), Allodynia Symptom Checklist, Photosensitivity Assessment Questionnaire, Beck Depression Inventory (BDI), State-Trait Anxiety Inventory, Post-Traumatic Stress Disorder (PTSD) checklist, Ray Auditory Verbal Learning Test, and the Trail Making Test A and B to assess headache characteristics, disability, insomnia symptoms, sensory hypersensitivities, and neuropsychological factors. Fisher's test and one-way ANOVA or Tukey's Honest Significant Difference were used to assess group differences of categorical and continuous data. Stepwise linear regression analyses were conducted to identify clinical variables associated with insomnia symptoms.
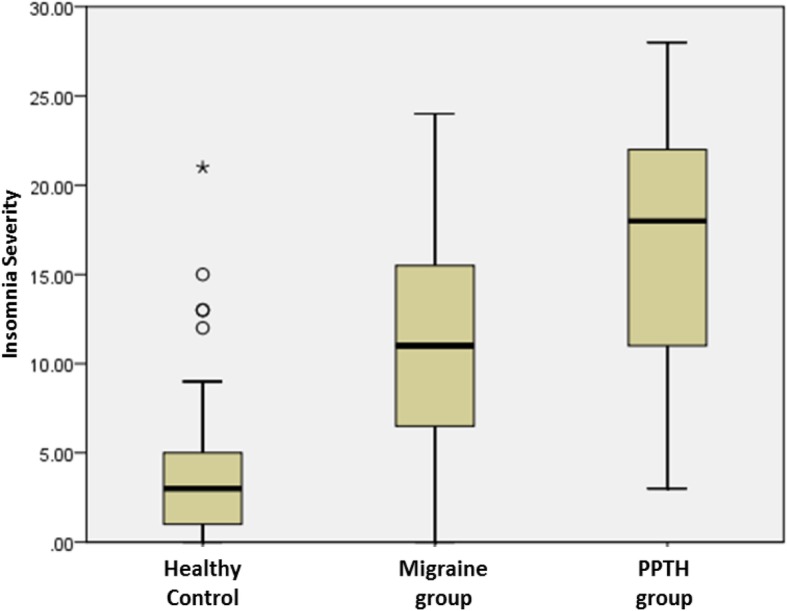
Those with PPTH had significantly higher ISI scores (16.7 ± 6.6) compared to migraine patients (11.3 ± 6.4) and healthy controls (4.1 ± 4.8) (p < 0.001). For those with PPTH, insomnia severity was most strongly correlated with the BDI (Spearman's rho (ρ) = 0.634, p < 0.01), followed by Trait Anxiety (ρ = 0.522, p < 0.01), PTSD (ρ = 0.505, p < 0.01), HQ (ρ = 0.469, p < 0.01), State Anxiety (ρ = 0.437, p < 0.01), and MIDAS scores (ρ = 0.364, p < 0.01). According to linear regression models, BDI, headache intensity, and hyperacusis scores were significantly positively associated with insomnia severity in those with PPTH, while only delayed memory recall was negatively associated with insomnia severity in those with migraine.
Insomnia symptoms were more severe in those with PPTH compared to migraine and healthy control cohorts. Depression, headache intensity, and hyperacusis were associated with insomnia in individuals with PPTH. Future studies should determine the bidirectional impact of treating insomnia and its associated symptoms.
在偏头痛患者中,已经确定了失眠与其他临床因素之间的密切关联,但很少有研究调查持续性创伤后头痛(PPTH)患者的失眠与临床因素之间的关系。本研究的目的是比较 PPTH、偏头痛和健康对照组中失眠症状的严重程度,并确定与 PPTH 患者失眠相关的因素与偏头痛患者失眠相关的因素。
在这项横断面队列研究中,纳入了 57 名归因于轻度创伤性脑损伤的 PPTH 患者、39 名偏头痛患者和 39 名健康对照组。参与者完成了详细的头痛特征问卷、偏头痛残疾评估量表(MIDAS)、失眠严重程度指数(ISI)、听觉过敏问卷(HQ)、感觉异常症状检查表、光过敏评估问卷、贝克抑郁量表(BDI)、状态-特质焦虑量表、创伤后应激障碍(PTSD)检查表、雷氏听觉言语学习测验和连线测验 A 和 B,以评估头痛特征、残疾、失眠症状、感觉敏感性和神经心理学因素。Fisher 检验和单向方差分析或 Tukey 的诚实显著差异用于评估分类和连续数据的组间差异。进行逐步线性回归分析以确定与失眠症状相关的临床变量。
与偏头痛患者(11.3±6.4)和健康对照组(4.1±4.8)相比,PPTH 患者的 ISI 评分(16.7±6.6)显著更高(p<0.001)。对于那些患有 PPTH 的人来说,失眠的严重程度与 BDI 的相关性最强(Spearman's rho(ρ)=0.634,p<0.01),其次是特质焦虑(ρ=0.522,p<0.01),PTSD(ρ=0.505,p<0.01),HQ(ρ=0.469,p<0.01),状态焦虑(ρ=0.437,p<0.01)和 MIDAS 评分(ρ=0.364,p<0.01)。根据线性回归模型,BDI、头痛强度和听觉过敏评分与 PPTH 患者的失眠严重程度呈显著正相关,而偏头痛患者中只有延迟记忆回忆与失眠严重程度呈负相关。
与偏头痛和健康对照组相比,PPTH 患者的失眠症状更为严重。抑郁、头痛强度和听觉过敏与 PPTH 患者的失眠相关。未来的研究应确定治疗失眠及其相关症状的双向影响。