Smith Andrea L, Watts Caroline G, Robinson Samuel, Schmid Helen, Chang Chiao-Han, Thompson John F, Rapport Frances, Cust Anne E
Research Fellow, Australian Institute of Health Innovation, Macquarie University, Sydney, Australia
Melanoma Institute Australia, Sydney, Australia.
BJGP Open. 2020 Jun 23;4(2). doi: 10.3399/bjgpopen20X101028. Print 2020.
In Australia, melanoma is managed in primary and secondary care settings. An individual concerned about a suspicious lesion typically presents first to their GP.
To identify factors influencing GPs' decisions to diagnose, treat, or refer patients with suspected melanoma.
DESIGN & SETTING: Semi-structured interviews were undertaken with 23 GPs working in general practice or skin cancer clinics in Australia.
The semi-structured interviews were audio-recorded, de-identified, and professionally transcribed. Thematic analysis was used to analyse the data.
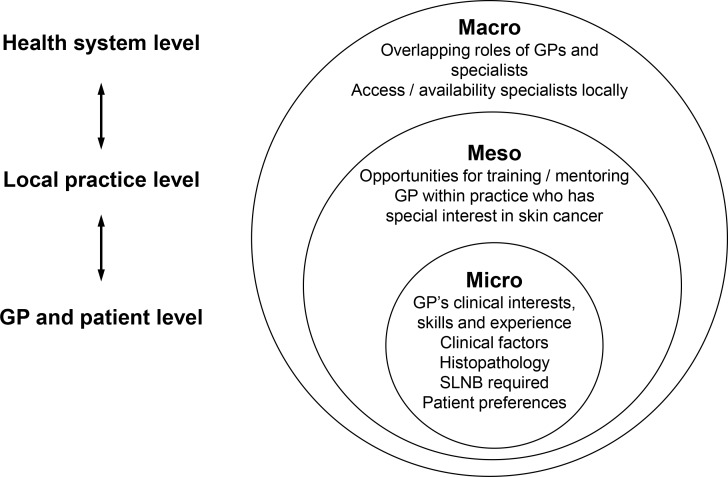
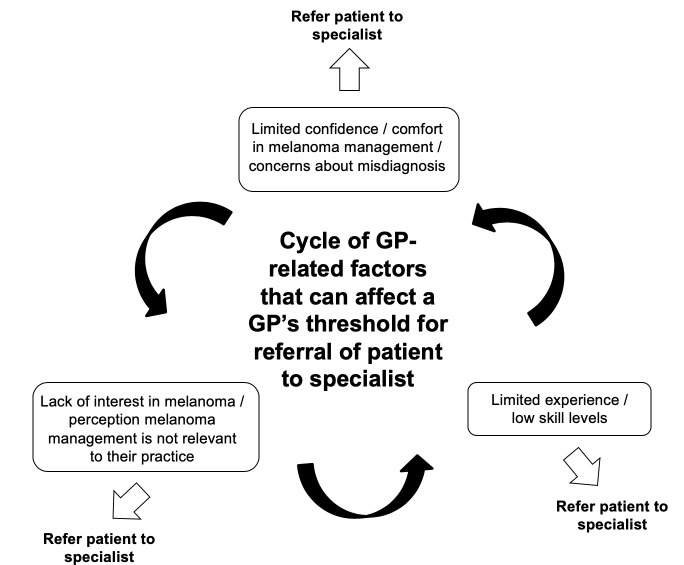
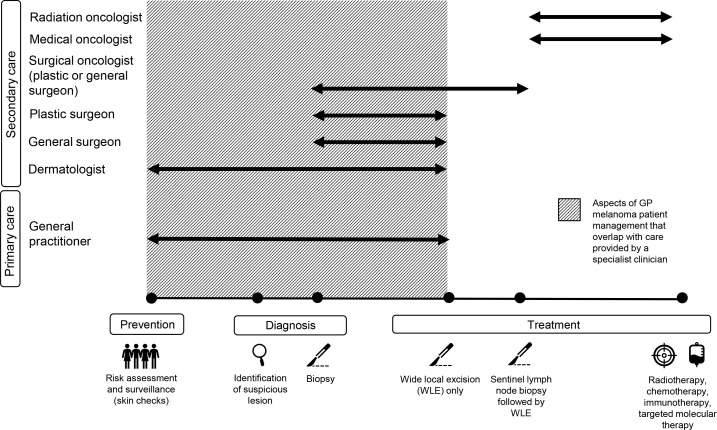
Considerable variation existed in GPs' self-reported confidence and involvement in melanoma management. Multiple factors were identified as influencing GPs' decisions to diagnose, treat, or refer patients with suspected or confirmed melanoma. Health system level factors included the overlapping roles of GPs and specialists, and access to and/or availability of specialists. Practice level factors included opportunities for formal and informal training, and having a GP with a special interest in skin cancer within their practice. GP and patient level factors included the GP's clinical interests, the clinical features (for example, site and size) and histopathology of the suspected melanoma, eligibility for possible sentinel lymph node biopsy, and patient preferences. For some GPs, concerns over misdiagnosis and the option of referring patients at any stage in the melanoma management continuum appeared to affect their interest and confidence in melanoma management.
GP involvement in melanoma patient care can extend well beyond cancer screening, prevention and supportive care roles to include provision of definitive melanoma patient management. GPs with an interest in being involved in melanoma management should be encouraged and supported to develop the skills needed to manage these patients, and to refer when appropriate.
在澳大利亚,黑色素瘤在初级和二级医疗环境中进行管理。担心有可疑病变的个人通常首先会去看他们的全科医生(GP)。
确定影响全科医生对疑似黑色素瘤患者进行诊断、治疗或转诊决策的因素。
对在澳大利亚从事全科医疗或皮肤癌诊所工作的23名全科医生进行了半结构化访谈。
半结构化访谈进行了录音、去识别化处理,并由专业人员进行转录。采用主题分析法对数据进行分析。
全科医生自我报告的在黑色素瘤管理方面的信心和参与程度存在很大差异。确定了多个因素影响全科医生对疑似或确诊黑色素瘤患者进行诊断、治疗或转诊的决策。卫生系统层面的因素包括全科医生和专科医生角色的重叠,以及专科医生的可及性和/或可用性。诊所层面的因素包括正式和非正式培训的机会,以及诊所内有对皮肤癌有特殊兴趣的全科医生。全科医生和患者层面的因素包括全科医生的临床兴趣、疑似黑色素瘤的临床特征(如部位和大小)及组织病理学、是否符合前哨淋巴结活检条件以及患者偏好。对于一些全科医生来说,对误诊的担忧以及在黑色素瘤管理连续过程中任何阶段转诊患者的选择似乎影响了他们对黑色素瘤管理的兴趣和信心。
全科医生对黑色素瘤患者的护理参与可以远远超出癌症筛查、预防和支持性护理角色,包括提供确定性的黑色素瘤患者管理。应鼓励和支持有兴趣参与黑色素瘤管理的全科医生发展管理这些患者所需的技能,并在适当的时候进行转诊。