Department of Global Health, University of Washington, Seattle, USA.
Departments of Medicine and Global Health, University of Washington, Seattle, USA.
BMC Infect Dis. 2020 Apr 16;20(1):283. doi: 10.1186/s12879-020-04978-9.
Haiti initiated the scale-up of HIV viral load (VL) testing in 2015-2016, with plans to achieve 100% coverage for all patients on antiretroviral therapy (ART) for treatment of HIV/AIDS. In the absence of HIV drug susceptibility testing, VL testing is a key tool for monitoring response to ART and optimizing treatment results. This study describes trends in expanded use of VL testing, VL results, and use of second-line ART regimens, and explores the association between VL testing and second-line regimen switching in Haiti from 2010 to 2017.
We conducted a retrospective cohort study with 66,042 patients drawn from 88 of Haiti's 160 national ART clinics. Longitudinal data from the iSanté electronic data system was used to analyze the trends of interest. We described patients' VL testing status in five categories based on up to two most recent VL test results: no test; suppressed; unsuppressed followed by no test; re-suppressed; and confirmed failure. Among those with confirmed failure, we described ART adherence level. Finally, we used Cox proportional hazards regression to estimate the risk of second-line regimen switching by VL testing status, after adjusting for other individual characteristics.
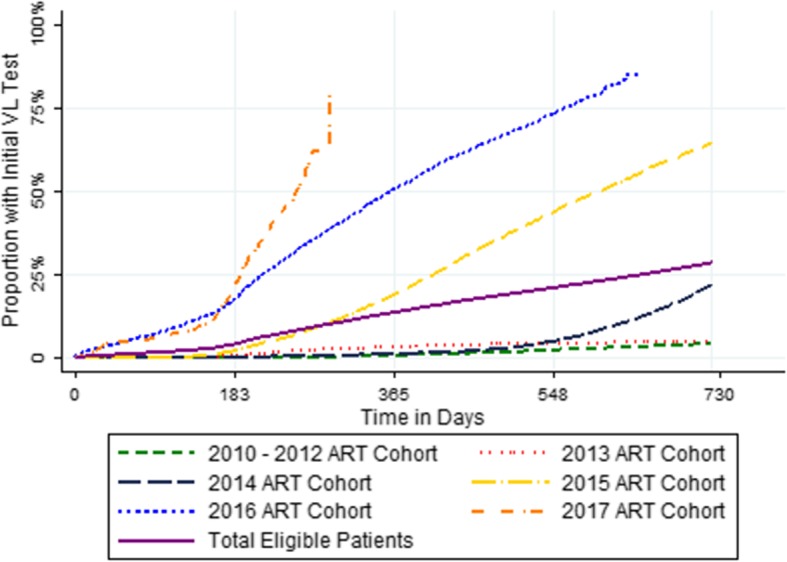
The number of patients who had tests done increased annually from 11 in 2010 to 18,828 in the first 9 months of 2017, while the number of second-line regimen switches rose from 21 to 279 during this same period. Compared with patients with no VL test, the hazard ratio (HR) for switching to a second-line regimen was 22.2 for patients with confirmed VL failure (95% confidence interval [CI] for HR: 18.8-26.3; p < 0.005) after adjustment for individual characteristics. Among patients with confirmed VL failure, 44.7% had strong adherence, and fewer than 20% of patients switched to a second-line regimen within 365 days of VL failure.
Haiti has significantly expanded access to VL testing since 2016. In order to promote optimal patient health outcomes, it is essential for Haiti to continue broadening access to confirmatory VL testing, to expand evidence-based initiatives to promote strong ART adherence, and to embrace timely switching for patients with confirmed ART failure despite strong ART adherence.
海地于 2015-2016 年开始扩大艾滋病毒病毒载量(VL)检测规模,计划为所有接受抗逆转录病毒疗法(ART)治疗艾滋病毒/艾滋病的患者实现 100%的覆盖率。在缺乏 HIV 药物敏感性检测的情况下,VL 检测是监测 ART 反应和优化治疗效果的关键工具。本研究描述了 2010 年至 2017 年期间海地扩大 VL 检测、VL 结果和二线 ART 方案使用的趋势,并探讨了 VL 检测与海地二线方案转换之间的关联。
我们对来自海地 160 个国家 ART 诊所中的 88 个诊所的 66042 名患者进行了回顾性队列研究。使用 iSanté 电子数据系统的纵向数据来分析感兴趣的趋势。我们根据最近两次 VL 检测结果将患者的 VL 检测状态分为五类:无检测、抑制、抑制后无检测、再抑制和确认失败。在确认失败的患者中,我们描述了 ART 依从性水平。最后,我们使用 Cox 比例风险回归估计了根据其他个体特征调整后,根据 VL 检测状态转换为二线方案的风险。
每年接受检测的患者人数从 2010 年的 11 人增加到 2017 年前 9 个月的 18828 人,而同期二线方案转换人数从 21 人增加到 279 人。与未进行 VL 检测的患者相比,在调整了个体特征后,VL 确认失败的患者转换为二线方案的风险比(HR)为 22.2(95%置信区间[HR]:18.8-26.3;p<0.005)。在 VL 确认失败的患者中,44.7% 的患者具有较强的依从性,并且在 VL 失败后 365 天内不到 20%的患者转换为二线方案。
自 2016 年以来,海地已显著扩大了对 VL 检测的获取。为了促进患者的最佳健康结果,海地必须继续扩大确认性 VL 检测的获取,扩大基于证据的举措以促进强有力的 ART 依从性,并在确认 ART 失败的患者中及时进行转换,尽管这些患者具有较强的 ART 依从性。