Department of Molecular Cell Biology and Immunology, Amsterdam Infection & Immunity Institute and Cancer Center Amsterdam, Amsterdam UMC, Vrije Universiteit Amsterdam, Amsterdam, The Netherlands
Department of Molecular Cell Biology and Immunology, Amsterdam Infection & Immunity Institute and Cancer Center Amsterdam, Amsterdam UMC, Vrije Universiteit Amsterdam, Amsterdam, The Netherlands.
J Immunother Cancer. 2020 Apr;8(1). doi: 10.1136/jitc-2019-000323.
Glioblastoma (GBM) is the most common and deadliest form of brain cancer in adults. Standard treatment, consisting of surgery and radiochemotherapy, only provides a modest survival benefit and is incapable of combating infiltrating GBM cells in other parts of the brain. New therapies in clinical trials, such as anti-programmed cell death 1 immunotherapy, have so far shown limited success in GBM. Moreover, it is unclear how the growth of GBM suppresses the immune system locally at the site of the brain tumor or if distant sites of tumor cell migration are also involved. Invasive GBM cells in brain tissue beyond the primary tumor limit the use of surgery, thus immunotherapy could be beneficial if activated/suppressed immune cells are present in the contralateral hemisphere.
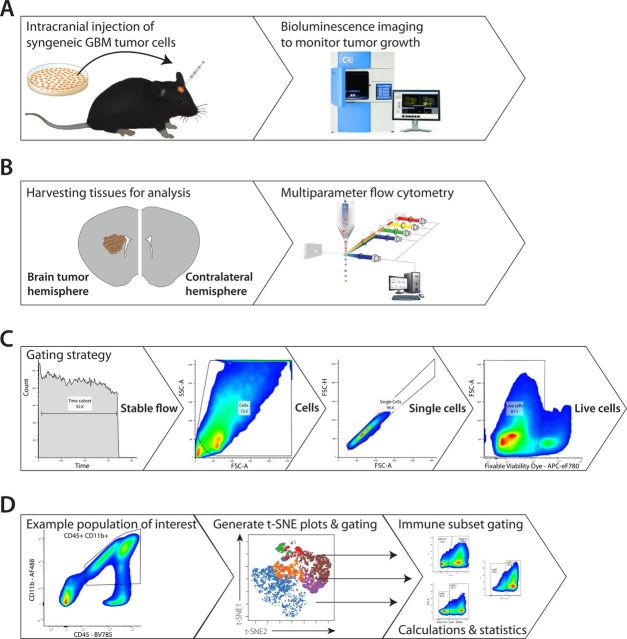
Here, we used a syngeneic orthotopic GL26 GBM mouse model and multiparameter fluorescence-activated cell sorting analysis to study the phenotype of resident and infiltrating immune cells in both the brain tumor hemisphere and contralateral hemisphere.
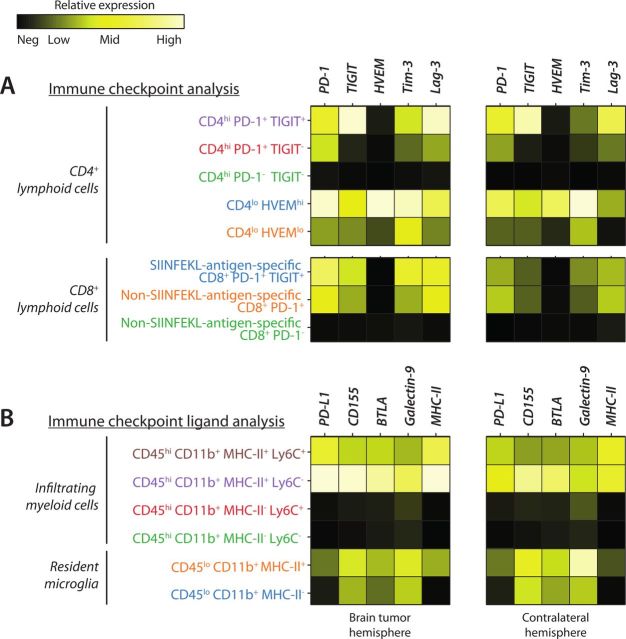
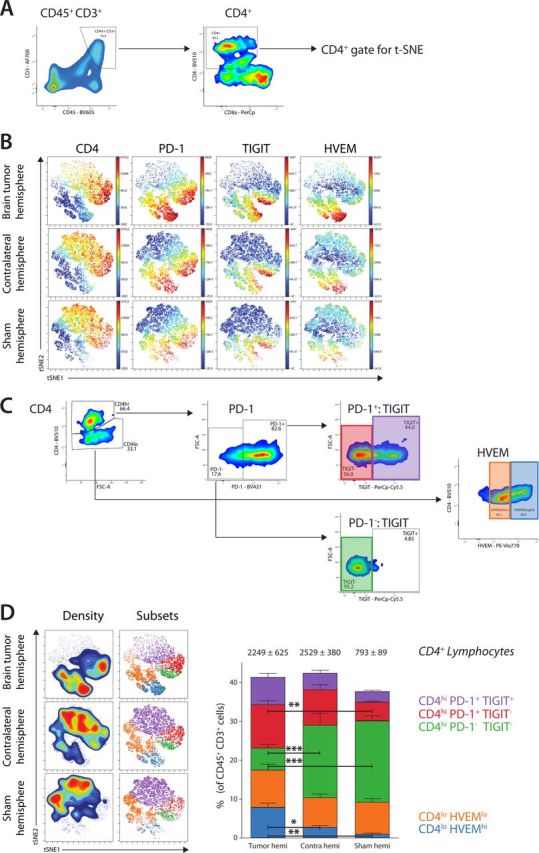
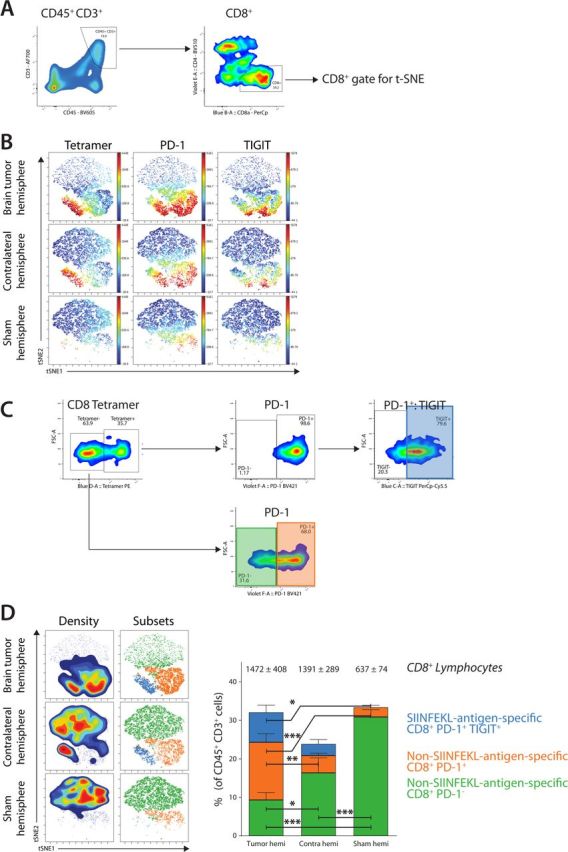
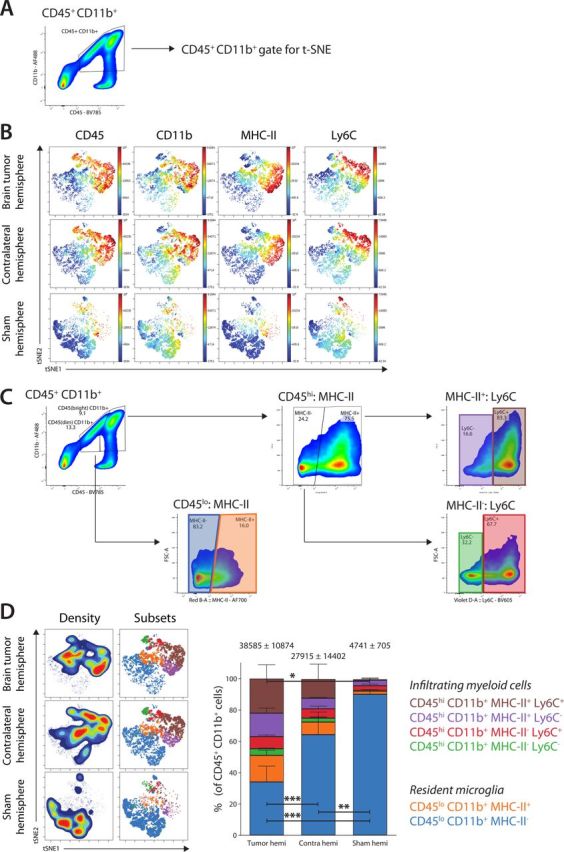
We show that lymphoid cells, including tumor antigen-specific CD8 tumor-infiltrating lymphocytes (TILs) are present in the tumor and are characterized by a tolerogenic phenotype based on high immune checkpoint expression. Massive infiltration of myeloid cells is observed, expressing immune checkpoint ligands, suggesting an immune-dependent coinhibitory axis limiting TIL responses. Surprisingly, these phenotypes are paralleled in the contralateral hemisphere, showing that infiltrating immune cells are also present at distant sites, expressing key immune checkpoints and immune checkpoint ligands.
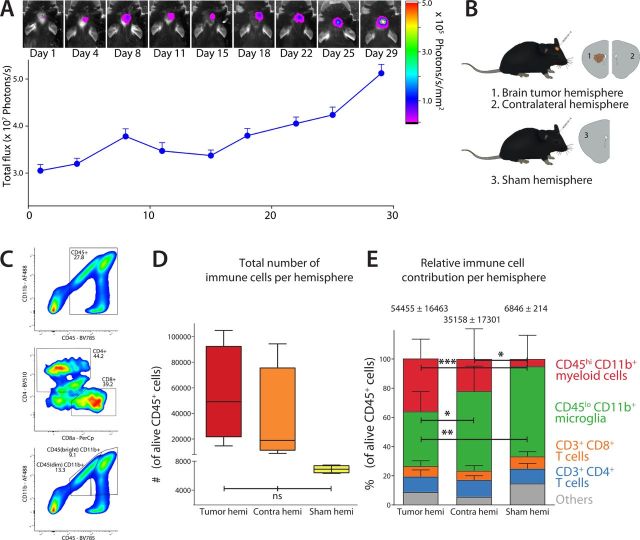
Whole-brain analysis indicates active immune involvement throughout the brain, both at the site of the primary tumor and in the contralateral hemisphere. Using the right combination and timing, immune checkpoint blockade could have the potential to activate immune cells at the site of the brain tumor and at distant sites, thereby also targeting diffusely infiltrating GBM cells.
胶质母细胞瘤(GBM)是成人中最常见和最致命的脑癌形式。由手术和放化疗组成的标准治疗方法仅提供适度的生存益处,并且无法对抗大脑其他部位浸润性 GBM 细胞。临床试验中的新疗法,如抗程序性细胞死亡 1 免疫疗法,迄今为止在 GBM 中的疗效有限。此外,尚不清楚 GBM 的生长如何在脑肿瘤部位局部抑制免疫系统,或者肿瘤细胞迁移的远处部位是否也参与其中。原发性肿瘤以外的脑组织中的浸润性 GBM 细胞限制了手术的应用,因此,如果在对侧半球存在激活/抑制的免疫细胞,免疫疗法可能会有益。
在这里,我们使用了同源原位 GL26 GBM 小鼠模型和多参数荧光激活细胞分选分析来研究大脑肿瘤半球和对侧半球中驻留和浸润免疫细胞的表型。
我们表明,淋巴细胞,包括肿瘤抗原特异性 CD8 肿瘤浸润淋巴细胞(TIL)存在于肿瘤中,并基于高免疫检查点表达表现出耐受性表型。大量浸润的髓样细胞表达免疫检查点配体,表明存在依赖免疫的共抑制轴限制 TIL 反应。令人惊讶的是,这些表型在对侧半球中也存在,表明浸润性免疫细胞也存在于远处部位,表达关键的免疫检查点和免疫检查点配体。
全脑分析表明,整个大脑都存在活跃的免疫参与,包括原发性肿瘤部位和对侧半球。通过正确的组合和时机,免疫检查点阻断有可能在脑肿瘤部位和远处部位激活免疫细胞,从而也靶向弥漫浸润性 GBM 细胞。