Division of Cardiovascular Disease, University of Alabama at Birmingham, Birmingham, Alabama.
Department of Medicine, University of Alabama at Birmingham, Birmingham, Alabama.
Am J Cardiol. 2020 Jun 15;125(12):1870-1878. doi: 10.1016/j.amjcard.2020.03.006. Epub 2020 Mar 16.
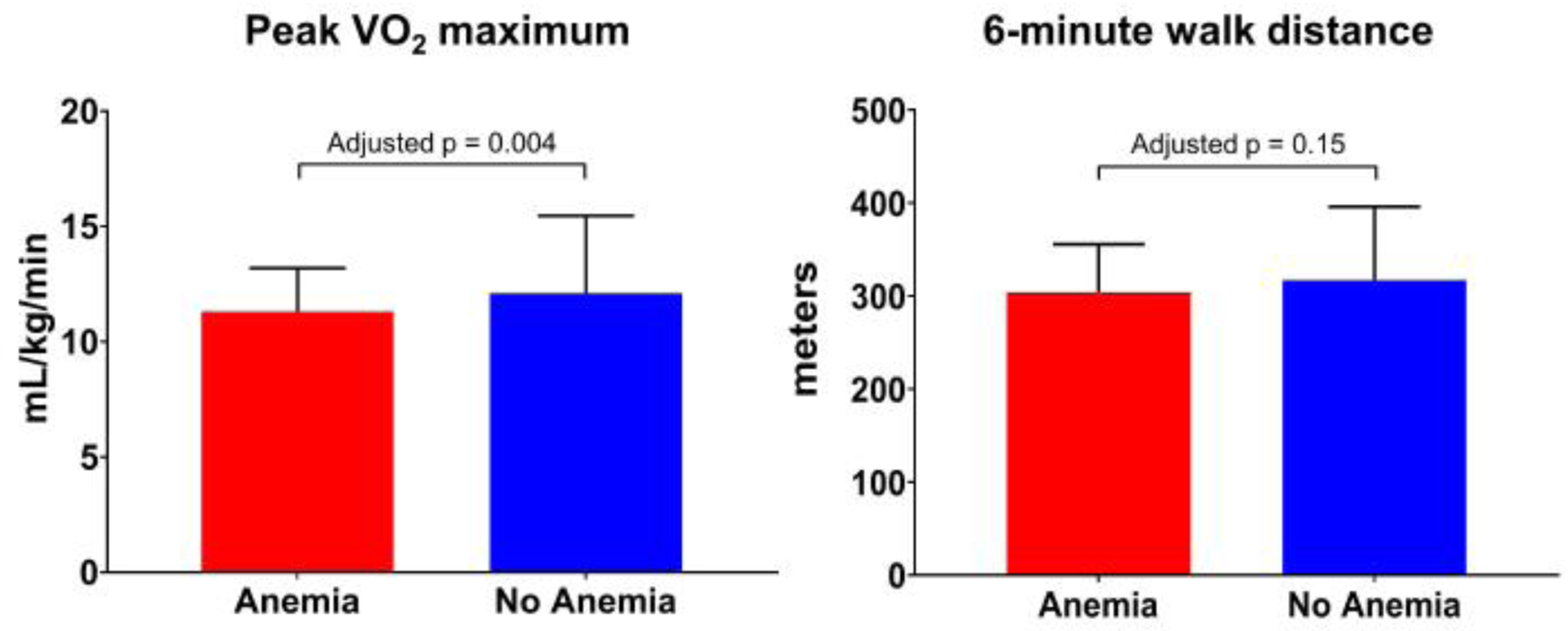
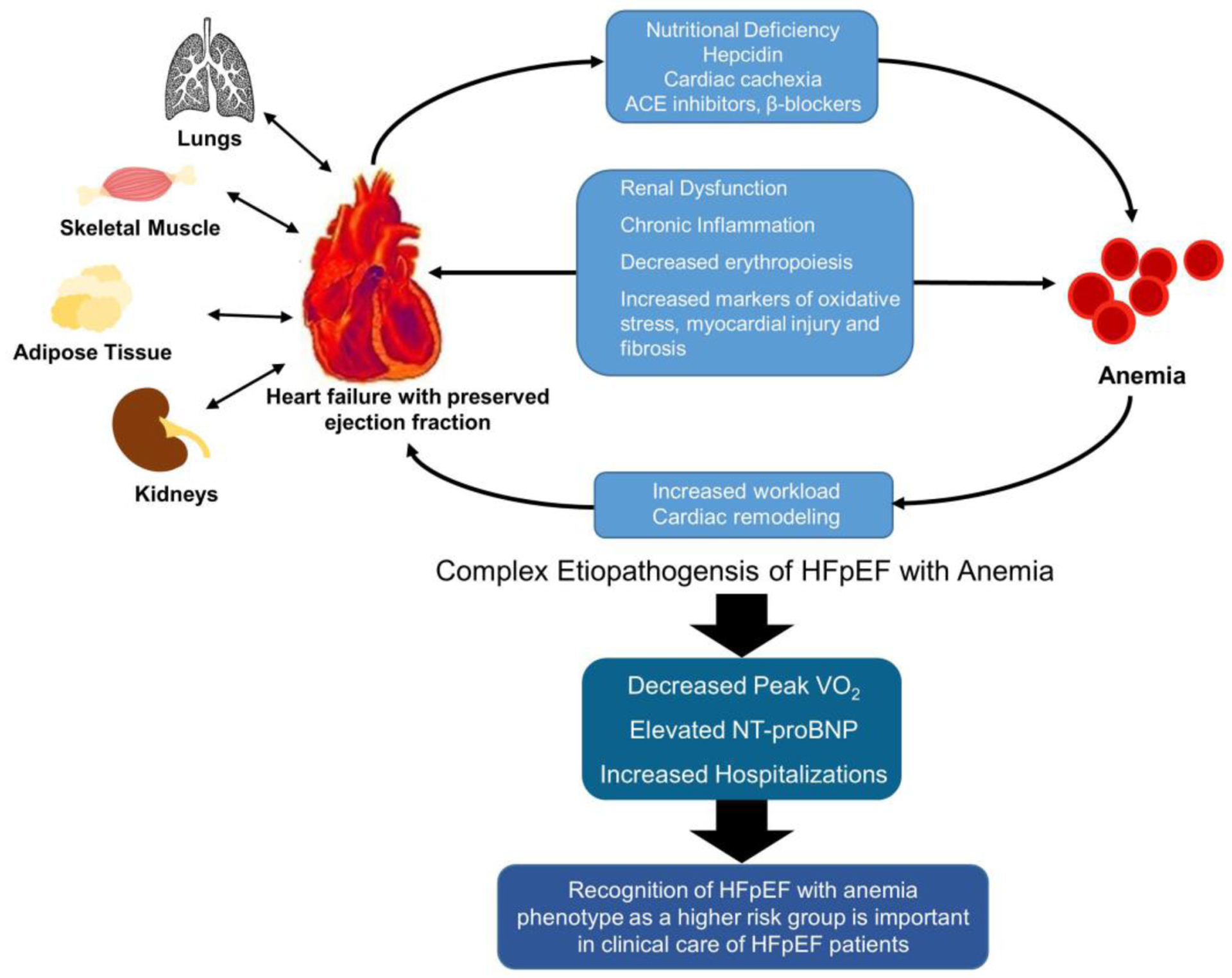
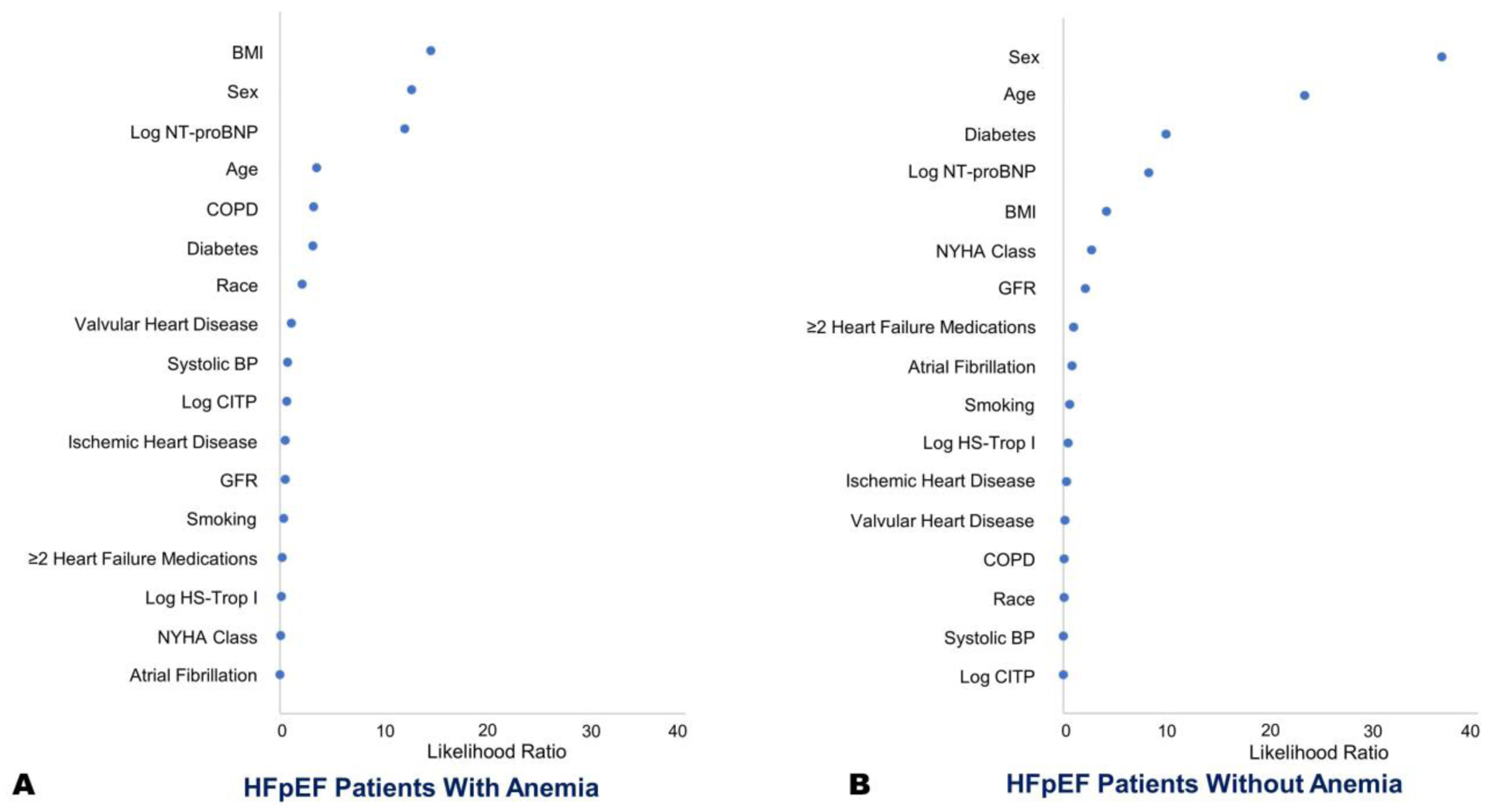
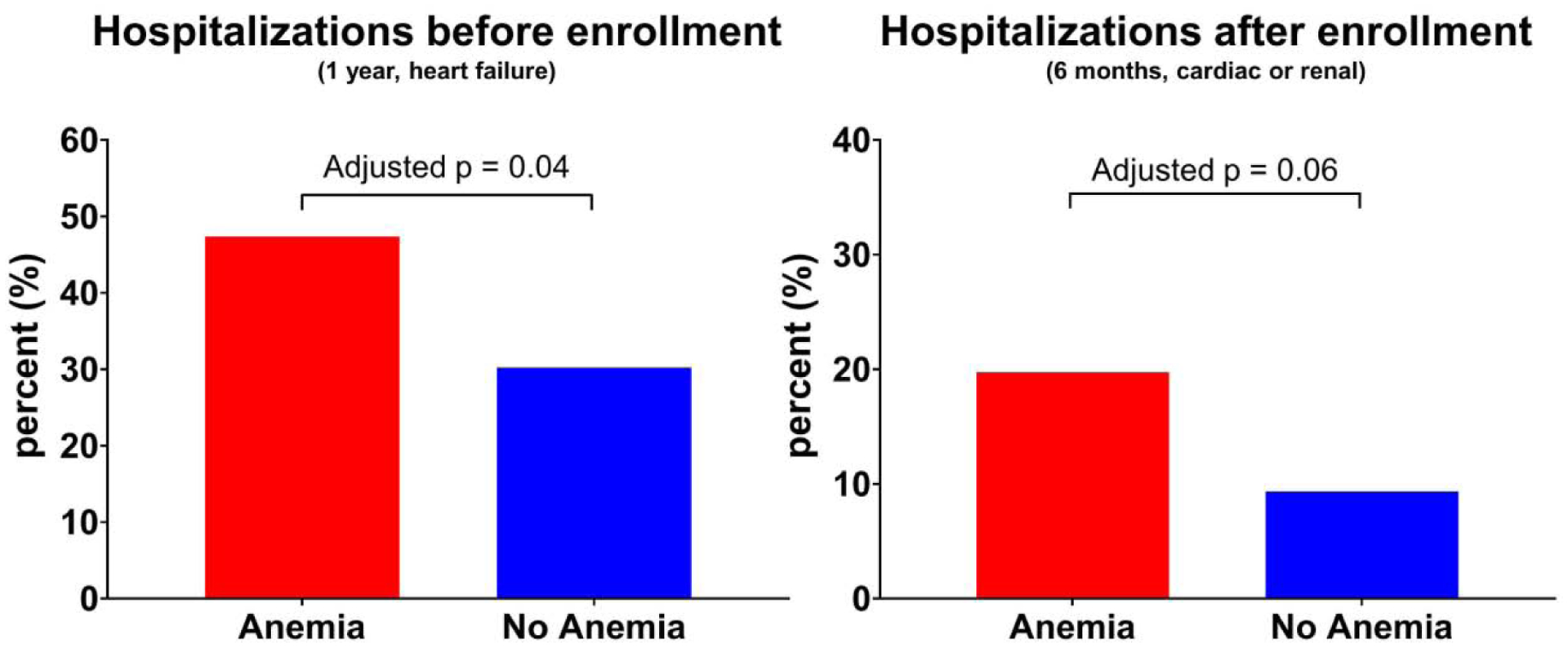
Anemia is a commonly occurring comorbidity among patients of heart failure with preserved ejection fraction (HFpEF) but limited data exists on the cardiovascular phenotype of anemia in HFpEF. We sought to characterize the clinical features, exercise capacity, and outcomes in patients with HFpEF to elucidate the phenotype and pathophysiology of anemia in HFpEF. Post hoc analyses of participants enrolled in the RELAX (Phosphodiesterase-5 Inhibition to Improve Clinical Status and Exercise Capacity in Diastolic Heart Failure) trial was performed. Anemia was defined as hemoglobin <13 g/dL in men and <12 g/dL in women. Multivariate adjusted regression modeling was done to assess for differences in peak oxygen uptake. Adjusted hazard ratios were generated to assess difference in hospitalization events using a Cox proportional hazards model. Anemic HFpEF patients were more likely to be older, male, and have worse renal function (p <0.05 for all). N-terminal pro-B-type natriuretic peptide, troponin I, pro-collagen III N-terminal peptide, C-telopeptide for type I collagen, uric acid, cystatin-c, and galectin-3 (p <0.05 for all) levels were higher in anemic HFpEF patients. In adjusted models, anemic HFpEF patients had worse exercise capacity (peak oxygen uptake: 11.3 vs 12.1 mL/kg/min; p = 0.004). The hazard for cardiac or renal cause of hospitalization in those with anemia was 2.0 (95% confidence interval: 0.9 to 4.3). Anemic HFpEF patients have worse exercise capacity and are more likely to be hospitalized. A better understanding of the physiologic phenotypes of HFpEF patients may allow for greater personalization of treatment and prognostication in HFpEF patients.
贫血是射血分数保留的心力衰竭(HFpEF)患者中常见的合并症,但关于 HFpEF 中贫血的心血管表型的数据有限。我们旨在描述 HFpEF 患者的临床特征、运动能力和结局,以阐明 HFpEF 中贫血的表型和病理生理学。对参加 RELAX(磷酸二酯酶-5 抑制改善舒张性心力衰竭患者的临床状况和运动能力)试验的参与者进行了事后分析。贫血定义为男性血红蛋白<13g/dL,女性血红蛋白<12g/dL。使用多变量调整回归模型评估峰值摄氧量的差异。使用 Cox 比例风险模型生成调整后的危险比,以评估住院事件的差异。贫血性 HFpEF 患者更可能年龄较大、男性和肾功能更差(所有 p<0.05)。N 末端脑利钠肽前体、肌钙蛋白 I、前胶原 III N 端肽、I 型胶原 C 端肽、尿酸、胱抑素-C 和半乳糖凝集素-3(所有 p<0.05)在贫血性 HFpEF 患者中水平更高。在调整后的模型中,贫血性 HFpEF 患者的运动能力更差(峰值摄氧量:11.3 与 12.1mL/kg/min;p=0.004)。贫血患者因心脏或肾脏原因住院的风险为 2.0(95%置信区间:0.9 至 4.3)。贫血性 HFpEF 患者的运动能力更差,更有可能住院。更好地了解 HFpEF 患者的生理表型可能允许更个性化地治疗和预测 HFpEF 患者的预后。