Department of Cardiovascular Medicine, Mayo Clinic, Rochester, MN (Y.N.V.R., M.O., M.M.R., B.A.B.).
Department of Health Sciences Research, Mayo Clinic, Jacksonville, FL (R.E.C.).
Circulation. 2018 Aug 28;138(9):861-870. doi: 10.1161/CIRCULATIONAHA.118.034646.
Diagnosis of heart failure with preserved ejection fraction (HFpEF) is challenging in euvolemic patients with dyspnea, and no evidence-based criteria are available. We sought to develop and then validate noninvasive diagnostic criteria that could be used to estimate the likelihood that HFpEF is present among patients with unexplained dyspnea to guide further testing.
Consecutive patients with unexplained dyspnea referred for invasive hemodynamic exercise testing were retrospectively evaluated. Diagnosis of HFpEF (case) or noncardiac dyspnea (control) was ascertained by invasive hemodynamic exercise testing. Logistic regression was performed to evaluate the ability of clinical findings to discriminate cases from controls. A scoring system was developed and then validated in a separate test cohort.
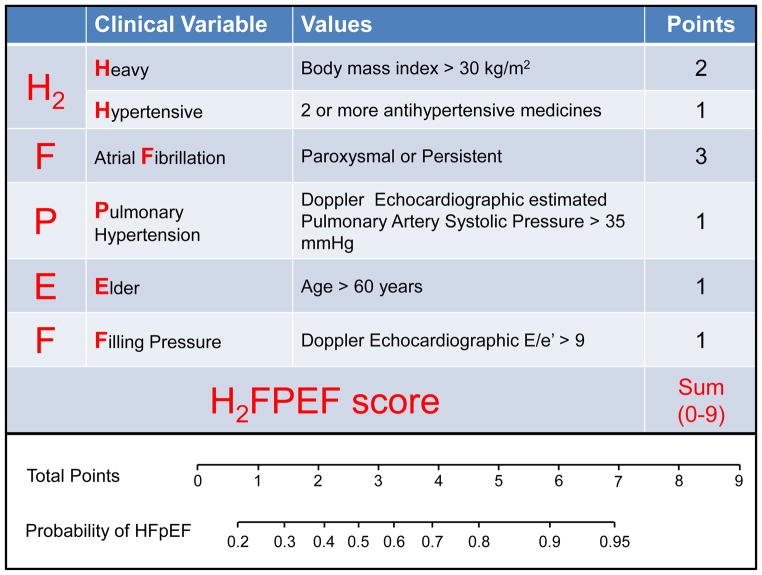
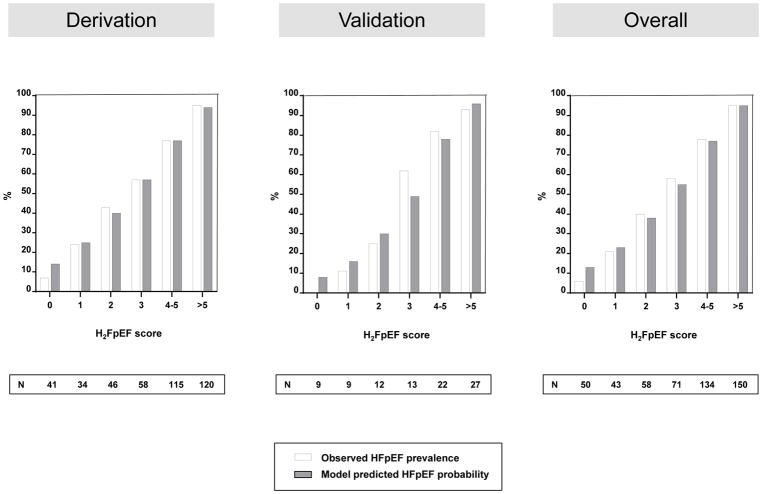
The derivation cohort included 414 consecutive patients (267 cases with HFpEF and 147 controls; HFpEF prevalence, 64%). The test cohort included 100 consecutive patients (61 with HFpEF; prevalence, 61%). Obesity, atrial fibrillation, age >60 years, treatment with ≥2 antihypertensives, echocardiographic E/e' ratio >9, and echocardiographic pulmonary artery systolic pressure >35 mm Hg were selected as the final set of predictive variables. A weighted score based on these 6 variables was used to create a composite score (HFPEF score) ranging from 0 to 9. The odds of HFpEF doubled for each 1-unit score increase (odds ratio, 1.98; 95% CI, 1.74-2.30; P<0.0001), with an area under the curve of 0.841 ( P<0.0001). The HFPEF score was superior to a currently used algorithm based on expert consensus (increase in area under the curve of 0.169; 95% CI, 0.120-0.217; P<0.0001). Performance in the independent test cohort was maintained (area under the curve, 0.886; P<0.0001).
The HFPEF score, which relies on simple clinical characteristics and echocardiography, enables discrimination of HFpEF from noncardiac causes of dyspnea and can assist in determination of the need for further diagnostic testing in the evaluation of patients with unexplained exertional dyspnea.
在容量正常的呼吸困难患者中,诊断射血分数保留的心力衰竭(HFpEF)具有挑战性,并且没有基于证据的标准。我们试图制定并验证非侵入性诊断标准,以便用于估计在不明原因呼吸困难的患者中存在 HFpEF 的可能性,从而指导进一步的检查。
回顾性评估连续因不明原因呼吸困难而接受有创血流动力学运动试验的患者。HFpEF(病例)或非心源性呼吸困难(对照)的诊断通过有创血流动力学运动试验确定。进行逻辑回归以评估临床发现区分病例与对照的能力。开发了一种评分系统,并在单独的测试队列中进行了验证。
该队列纳入了 414 例连续患者(267 例 HFpEF 病例和 147 例对照;HFpEF 患病率为 64%)。测试队列纳入了 100 例连续患者(61 例 HFpEF;患病率为 61%)。肥胖、心房颤动、年龄>60 岁、使用≥2 种降压药、超声心动图 E/e' 比值>9、超声心动图肺动脉收缩压>35mmHg 被选为最终的预测变量。基于这 6 个变量的加权评分创建了一个复合评分(HFPEF 评分),范围为 0 至 9。每增加 1 个单位评分,HFpEF 的可能性增加一倍(比值比,1.98;95%置信区间,1.74-2.30;P<0.0001),曲线下面积为 0.841(P<0.0001)。HFPEF 评分优于基于专家共识的当前使用的算法(曲线下面积增加 0.169;95%置信区间,0.120-0.217;P<0.0001)。在独立的测试队列中的性能保持不变(曲线下面积,0.886;P<0.0001)。
HFPEF 评分依赖于简单的临床特征和超声心动图,可用于区分 HFpEF 与非心源性呼吸困难的原因,并可帮助确定在评估不明原因运动性呼吸困难的患者时是否需要进一步的诊断性检查。