Department of Morphology, Surgery and Experimental Medicine, Section of Anaesthesia and Intensive Care, Azienda Ospedaliera-Universitaria Sant' Anna, University of Ferrara, 8, Aldo Moro, 44121, Ferrara, Italy.
Department of Intensive Care, Erasme Hospital, Université Libre de Bruxelles, Brussels, Belgium.
Crit Care. 2020 Apr 20;24(1):160. doi: 10.1186/s13054-020-2827-5.
Guidelines recommend a restrictive red blood cell transfusion strategy based on hemoglobin (Hb) concentrations in critically ill patients. We hypothesized that the arterial-venous oxygen difference (A-V O), a surrogate for the oxygen delivery to consumption ratio, could provide a more personalized approach to identify patients who may benefit from transfusion.
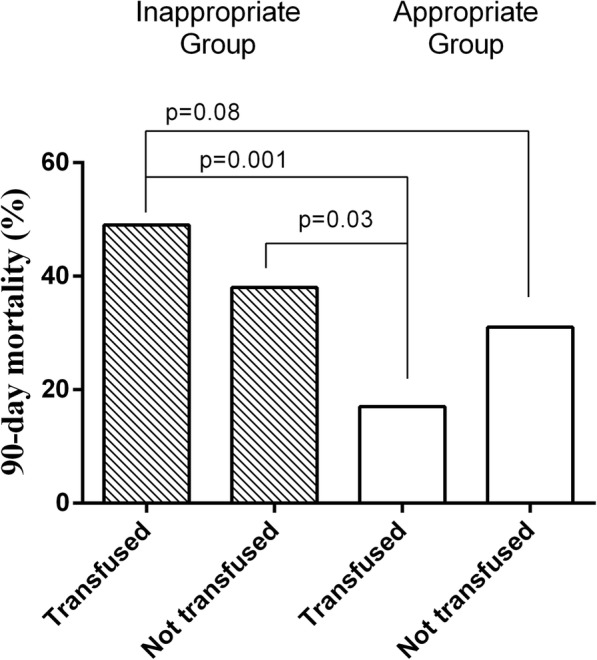
A prospective observational study including 177 non-bleeding adult patients with a Hb concentration of 7.0-10.0 g/dL within 72 h after ICU admission. The A-V O, central venous oxygen saturation (ScvO), and oxygen extraction ratio (OER) were noted when a patient's Hb was first within this range. Transfusion decisions were made by the treating physician according to institutional policy. We used the median A-V O value in the study cohort (3.7 mL) to classify the transfusion strategy in each patient as "appropriate" (patient transfused when the A-V O > 3.7 mL or not transfused when the A-V O ≤ 3.7 mL) or "inappropriate" (patient transfused when the A-V O ≤ 3.7 mL or not transfused when the A-V O > 3.7 mL). The primary outcome was 90-day mortality.
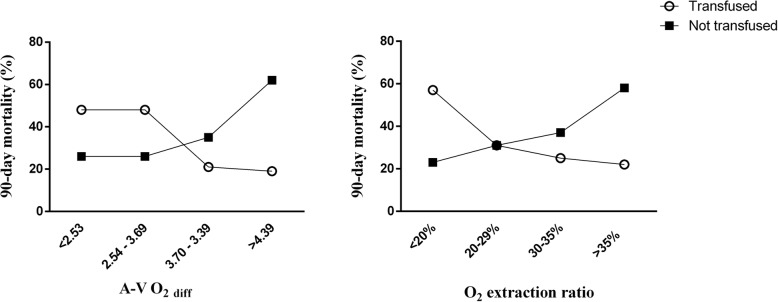
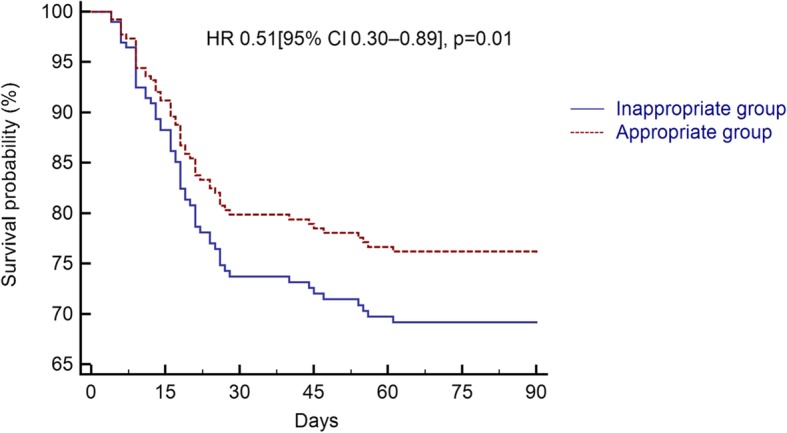
Patients managed with an "appropriate" strategy had lower mortality rates (23/96 [24%] vs. 36/81 [44%]; p = 0.004), and an "appropriate" strategy was independently associated with reduced mortality (hazard ratio [HR] 0.51 [95% CI 0.30-0.89], p = 0.01). There was a trend to less acute kidney injury with the "appropriate" than with the "inappropriate" strategy (13% vs. 26%, p = 0.06), and the Sequential Organ Failure Assessment (SOFA) score decreased more rapidly (p = 0.01). The A-V O, but not the ScvO, predicted 90-day mortality in transfused (AUROC = 0.656) and non-transfused (AUROC = 0.630) patients with moderate accuracy. Using the ROC curve analysis, the best A-V O cutoffs for predicting mortality were 3.6 mL in transfused and 3.5 mL in non-transfused patients.
In anemic, non-bleeding critically ill patients, transfusion may be associated with lower 90-day mortality and morbidity in patients with higher A-V O.
ClinicalTrials.gov, NCT03767127. Retrospectively registered on 6 December 2018.
指南建议根据危重症患者的血红蛋白(Hb)浓度采用限制性红细胞输血策略。我们假设动静脉氧差(A-V O),作为氧输送与消耗比值的替代指标,可以提供一种更个体化的方法来确定可能受益于输血的患者。
这是一项前瞻性观察性研究,纳入了 177 名非出血性成年患者,这些患者在 ICU 入院后 72 小时内 Hb 浓度为 7.0-10.0g/dL。当患者的 Hb 首次处于该范围内时,记录 A-V O、中心静脉血氧饱和度(ScvO)和氧摄取率(OER)。输血决策由主治医生根据机构政策做出。我们使用研究队列中的中位数 A-V O 值(3.7mL)将每个患者的输血策略分类为“适当”(当 A-V O>3.7mL 时患者输血,或当 A-V O≤3.7mL 时患者不输血)或“不适当”(当 A-V O≤3.7mL 时患者输血,或当 A-V O>3.7mL 时患者不输血)。主要结局为 90 天死亡率。
采用“适当”策略管理的患者死亡率较低(23/96[24%]比 36/81[44%];p=0.004),“适当”策略与降低死亡率独立相关(风险比[HR]0.51[95%CI 0.30-0.89],p=0.01)。与“不适当”策略相比,“适当”策略的急性肾损伤发生率较低(13%比 26%,p=0.06),序贯器官衰竭评估(SOFA)评分下降更快(p=0.01)。A-V O 而不是 ScvO 可以中等准确度预测输血(AUROC=0.656)和未输血(AUROC=0.630)患者的 90 天死亡率。使用 ROC 曲线分析,最佳的 A-V O 截断值用于预测死亡率的分别为 3.6mL 用于输血患者和 3.5mL 用于未输血患者。
在贫血且非出血的危重症患者中,较高的 A-V O 与输血患者较低的 90 天死亡率和发病率相关。
ClinicalTrials.gov,NCT03767127。于 2018 年 12 月 6 日进行回顾性注册。