Department of Cardiovascular Medicine, Saga University, Saga, Japan.
Department of Cardiology, Dokkyo Medical University Saitama Medical Center, Koshigaya, Japan.
PLoS Med. 2020 Apr 22;17(4):e1003095. doi: 10.1371/journal.pmed.1003095. eCollection 2020 Apr.
An elevated level of serum uric acid (SUA) is associated with an increased risk of cardiovascular disease. Pharmacological intervention with urate-lowering agents, such as the conventional purine analogue xanthine oxidase (XO) inhibitor, allopurinol, has been used widely for a long period of time in clinical practice to reduce SUA levels. Febuxostat, a novel non-purine selective inhibitor of XO, has higher potency for inhibition of XO activity and greater urate-lowering efficacy than conventional allopurinol. However, clinical evidence regarding the effects of febuxostat on atherosclerosis is lacking. The purpose of the study was to test whether treatment with febuxostat delays carotid intima-media thickness (IMT) progression in patients with asymptomatic hyperuricemia.
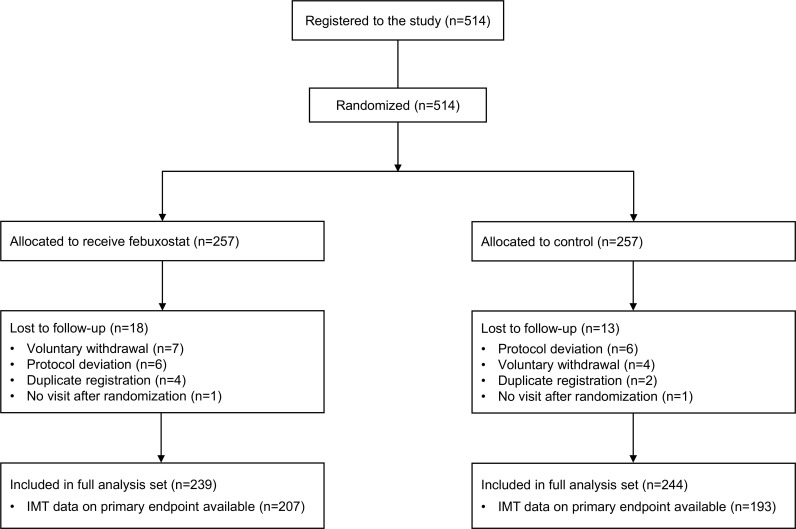
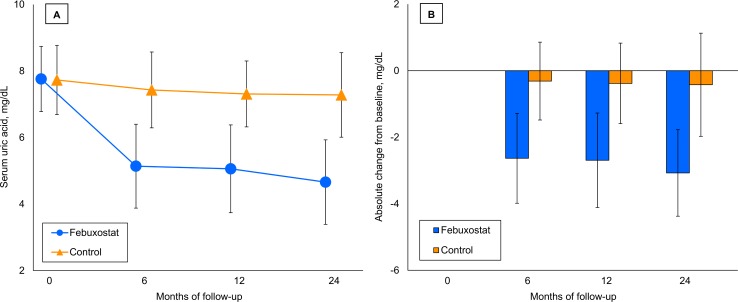
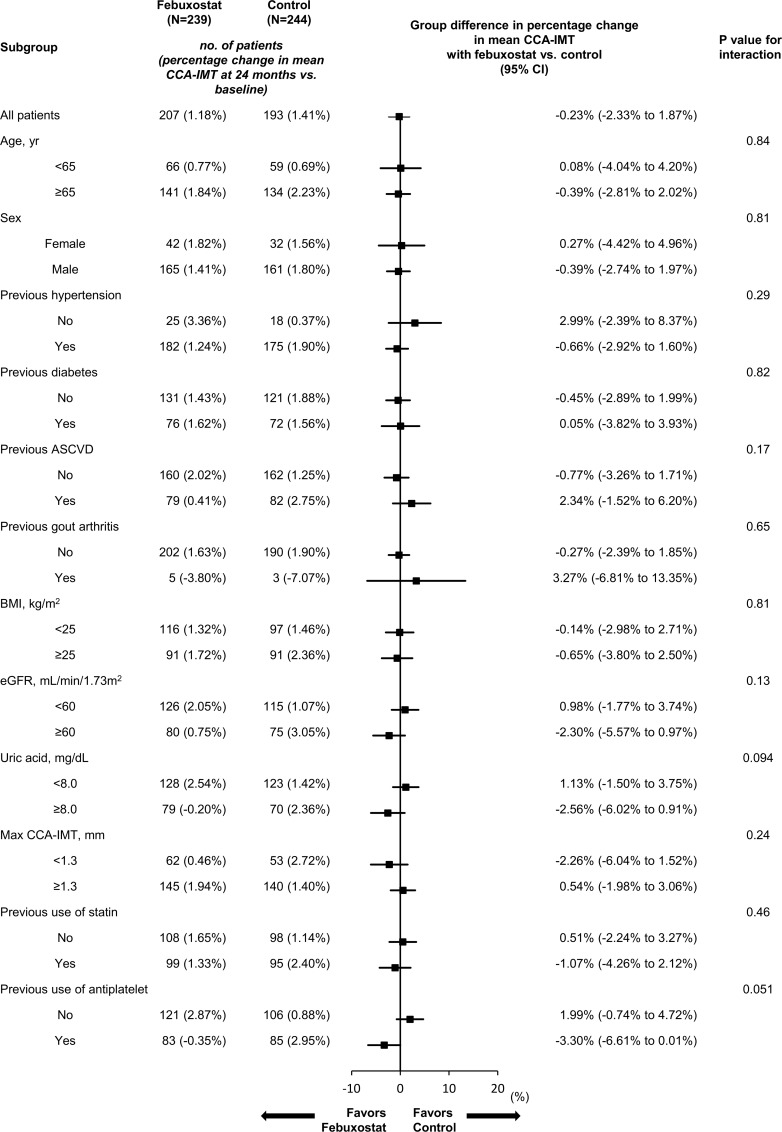
The study was a multicenter, prospective, randomized, open-label, blinded-endpoint clinical trial undertaken at 48 sites throughout Japan between May 2014 and August 2018. Adults with both asymptomatic hyperuricemia (SUA >7.0 mg/dL) and maximum IMT of the common carotid artery (CCA) ≥1.1 mm at screening were allocated equally using a central web system to receive either dose-titrated febuxostat (10-60 mg daily) or as a control-arm, non-pharmacological lifestyle modification for hyperuricemia, such as a healthy diet and exercise therapy. Of the 514 enrolled participants, 31 were excluded from the analysis, with the remaining 483 people (mean age 69.1 years [standard deviation 10.4 years], female 19.7%) included in the primary analysis (febuxostat group, 239; control group, 244), based on a modified intention-to-treat principal. The carotid IMT images were recorded by a single sonographer at each site and read in a treatment-blinded manner by a single analyzer at a central core laboratory. The primary endpoint was the percentage change from baseline to 24 months in mean IMT of the CCA, determined by analysis of covariance using the allocation adjustment factors (age, gender, history of type 2 diabetes, baseline SUA, and baseline maximum IMT of the CCA) as the covariates. Key secondary endpoints included changes in other carotid ultrasonographic parameters and SUA and the incidence of clinical events. The mean values (± standard deviation) of CCA-IMT were 0.825 mm ± 0.173 mm in the febuxostat group and 0.832 mm ± 0.175 mm in the control group (mean between-group difference [febuxostat - control], -0.007 mm [95% confidence interval (CI) -0.039 mm to 0.024 mm; P = 0.65]) at baseline; 0.832 mm ± 0.182 mm in the febuxostat group and 0.848 mm ± 0.176 mm in the control group (mean between-group difference, -0.016 mm [95% CI -0.051 mm to 0.019 mm; P = 0.37]) at 24 months. Compared with the control group, febuxostat had no significant effect on the primary endpoint (mean percentage change 1.2% [95% CI -0.6% to 3.0%] in the febuxostat group (n = 207) versus 1.4% [95% CI -0.5% to 3.3%] in the control group (n = 193); mean between-group difference, -0.2% [95% CI -2.3% to 1.9%; P = 0.83]). Febuxostat also had no effect on the other carotid ultrasonographic parameters. The mean baseline values of SUA were comparable between the two groups (febuxostat, 7.76 mg/dL ± 0.98 mg/dL versus control, 7.73 mg/dL ± 1.04 mg/dL; mean between-group difference, 0.03 mg/dL [95% CI -0.15 mg/dL to 0.21 mg/dL; P = 0.75]). The mean value of SUA at 24 months was significantly lower in the febuxostat group than in the control group (febuxostat, 4.66 mg/dL ± 1.27 mg/dL versus control, 7.28 mg/dL ± 1.27 mg/dL; mean between-group difference, -2.62 mg/dL [95% CI -2.86 mg/dL to -2.38 mg/dL; P < 0.001]). Episodes of gout arthritis occurred only in the control group (4 patients [1.6%]). There were three deaths in the febuxostat group and seven in the control group during follow-up. A limitation of the study was the study design, as it was not a placebo-controlled trial, had a relatively small sample size and a short intervention period, and only enrolled Japanese patients with asymptomatic hyperuricemia.
In Japanese patients with asymptomatic hyperuricemia, 24 months of febuxostat treatment did not delay carotid atherosclerosis progression, compared with non-pharmacological care. These findings do not support the use of febuxostat for delaying carotid atherosclerosis in this population.
University Hospital Medical Information Network Clinical Trial Registry UMIN000012911.
血清尿酸(SUA)水平升高与心血管疾病风险增加相关。长期以来,临床实践中一直使用黄嘌呤氧化酶(XO)抑制剂,如常规嘌呤类似物别嘌呤醇,来抑制尿酸生成,以降低 SUA 水平。非布司他是一种新型的选择性XO 抑制剂,对 XO 活性的抑制作用更强,降尿酸效果也更强。然而,关于非布司他对动脉粥样硬化影响的临床证据尚缺乏。本研究旨在检测在无症状高尿酸血症患者中,非布司他治疗是否能延缓颈动脉内膜中层厚度(IMT)进展。
该研究是一项多中心、前瞻性、随机、开放标签、盲终点临床试验,于 2014 年 5 月至 2018 年 8 月在日本 48 个地点进行。筛选时具有无症状高尿酸血症(SUA>7.0mg/dL)和颈总动脉(CCA)最大 IMT≥1.1mm 的成年人,通过中央网络系统等分为接受剂量滴定的非布司他(10-60mg/d)或作为对照组的非药物生活方式治疗高尿酸血症,如健康饮食和运动疗法。在 514 名入组患者中,31 名被排除在分析之外,其余 483 人(平均年龄 69.1 岁[标准差 10.4 岁],女性 19.7%)根据修改后的意向治疗主要原则纳入主要分析(非布司他组 239 例,对照组 244 例)。颈动脉 IMT 图像由每个站点的单个超声医师记录,并由中央核心实验室的单个分析人员以治疗盲方式进行读取。主要终点是由协方差分析确定的,使用分配调整因素(年龄、性别、2 型糖尿病史、基线 SUA 和 CCA 最大 IMT)作为协变量,从基线到 24 个月时 CCA 的平均 IMT 的百分比变化。关键次要终点包括其他颈动脉超声参数和 SUA 的变化以及临床事件的发生率。非布司他组和对照组的 CCA-IMT 平均值分别为 0.825mm±0.173mm和 0.832mm±0.175mm(组间平均差异[非布司他-对照组],-0.007mm[95%置信区间(CI)-0.039mm 至 0.024mm;P=0.65]);非布司他组和对照组的 CCA-IMT 平均值分别为 0.832mm±0.182mm和 0.848mm±0.176mm(组间平均差异,-0.016mm[95%CI-0.051mm 至 0.019mm;P=0.37])。与对照组相比,非布司他对主要终点无显著影响(非布司他组的平均百分比变化为 1.2%[95%CI-0.6%至 3.0%](n=207),对照组为 1.4%[95%CI-0.5%至 3.3%](n=193);组间平均差异,-0.2%[95%CI-2.3%至 1.9%;P=0.83])。非布司他对其他颈动脉超声参数也没有影响。两组的基线 SUA 均值相当(非布司他组 7.76mg/dL±0.98mg/dL,对照组 7.73mg/dL±1.04mg/dL;组间平均差异,0.03mg/dL[95%CI-0.15mg/dL 至 0.21mg/dL;P=0.75])。非布司他组的 SUA 均值在 24 个月时显著低于对照组(非布司他组 4.66mg/dL±1.27mg/dL,对照组 7.28mg/dL±1.27mg/dL;组间平均差异,-2.62mg/dL[95%CI-2.86mg/dL 至-2.38mg/dL;P<0.001])。只有对照组出现痛风性关节炎发作(4 例[1.6%])。在随访期间,非布司他组有 3 例死亡,对照组有 7 例死亡。该研究的一个局限性是研究设计,因为它不是安慰剂对照试验,样本量相对较小,干预时间较短,仅纳入了有无症状高尿酸血症的日本患者。
与非药物生活方式治疗相比,24 个月的非布司他治疗并未延缓日本无症状高尿酸血症患者的颈动脉粥样硬化进展。这些发现不支持在该人群中使用非布司他来延缓颈动脉粥样硬化。
日本大学医院医学信息网络临床试验注册 UMIN000012911。