Department of Radiology, Severance Hospital Stroke Center, Yonsei University College of Medicine, Seoul, Korea.
Department of Neurology, Keimyung University School of Medicine, Daegu, Korea.
Korean J Radiol. 2020 May;21(5):582-587. doi: 10.3348/kjr.2019.0578.
Endovascular thrombectomy (EVT) fails in approximately 20% of anterior circulation large vessel occlusion (AC-LVO). Nonetheless, the factors that affect clinical outcomes of non-recanalized AC-LVO despite EVT are less studied. The purpose of this study was to identify the factors affecting clinical outcomes in non-recanalized AC-LVO patients despite EVT.
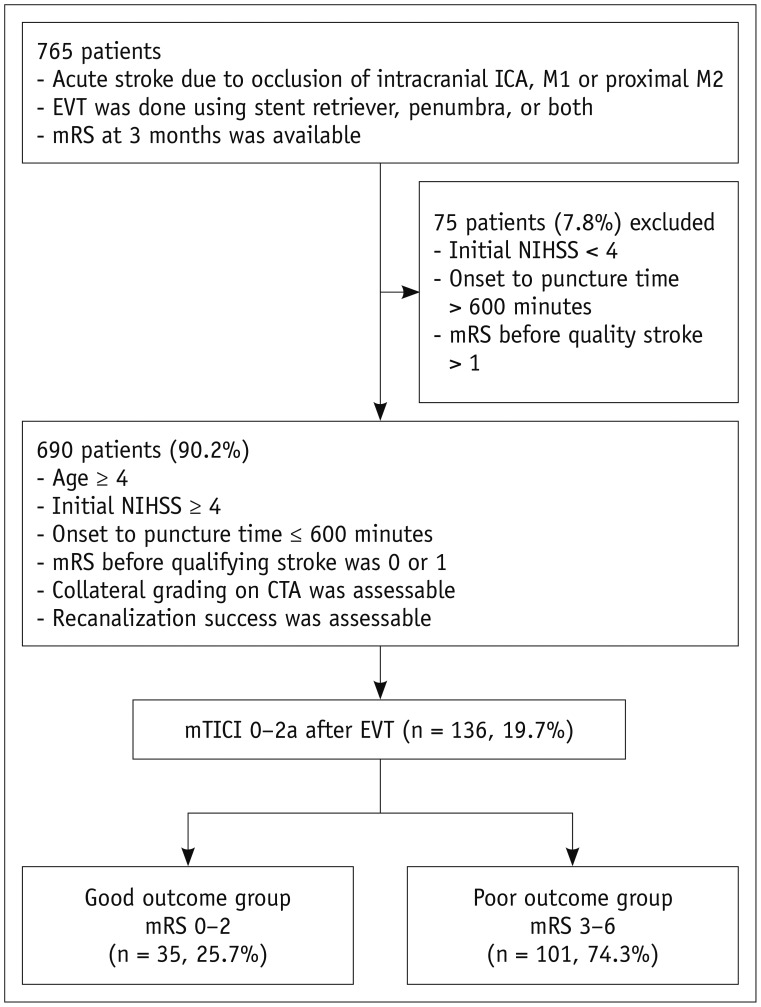
This was a retrospective analysis of clinical and imaging data from 136 consecutive patients who demonstrated recanalization failure (modified thrombolysis in cerebral ischemia [mTICI], 0-2a) despite EVT for AC-LVO. Data were collected in prospectively maintained registries at 16 stroke centers. Collateral status was categorized into good or poor based on the CT angiogram, and the mTICI was categorized as 0-1 or 2a on the final angiogram. Patients with good (modified Rankin Scale [mRS], 0-2) and poor outcomes (mRS, 3-6) were compared in multivariate analysis to evaluate the factors associated with a good outcome.
Thirty-five patients (25.7%) had good outcomes. The good outcome group was younger (odds ratio [OR], 0.962; 95% confidence interval [CI], 0.932-0.992; = 0.015), had a lower incidence of hypertension (OR, 0.380; 95% CI, 0.173-0.839; = 0.017) and distal internal carotid artery involvement (OR, 0.149; 95% CI, 0.043-0.520; = 0.003), lower initial National Institute of Health Stroke Scale (NIHSS) (OR, 0.789; 95% CI, 0.713-0.873; < 0.001) and good collateral status (OR, 13.818; 95% CI, 3.971-48.090; < 0.001). In multivariate analysis, the initial NIHSS (OR, 0.760; 95% CI, 0.638-0.905; = 0.002), good collateral status (OR, 14.130; 95% CI, 2.264-88.212; = 0.005) and mTICI 2a recanalization (OR, 5.636; 95% CI, 1.216-26.119; = 0.027) remained as independent factors with good outcome in non-recanalized patients.
Baseline NIHSS score, good collateral status, and mTICI 2a recanalization remained independently associated with clinical outcome in non-recanalized patients. mTICI 2a recanalization would benefit patients with good collaterals in non-recanalized AC-LVO patients despite EVT.
血管内血栓切除术(EVT)在大约 20%的前循环大血管闭塞(AC-LVO)患者中失败。尽管如此,EVT 后非再通的 AC-LVO 患者影响临床结局的因素研究较少。本研究旨在确定影响 EVT 后非再通的 AC-LVO 患者临床结局的因素。
这是一项对 136 例连续接受 EVT 治疗但出现再通失败(改良脑梗死溶栓试验[mTICI],0-2a)的 AC-LVO 患者的临床和影像学数据的回顾性分析。数据来自 16 个卒中中心前瞻性维护的登记处。根据 CT 血管造影将侧支循环状态分为良好或不良,根据最终血管造影将 mTICI 分为 0-1 或 2a。在多变量分析中比较良好结局(改良 Rankin 量表[mRS],0-2)和不良结局(mRS,3-6)患者,以评估与良好结局相关的因素。
35 例患者(25.7%)有良好结局。良好结局组年龄较小(比值比[OR],0.962;95%置信区间[CI],0.932-0.992; = 0.015),高血压发生率较低(OR,0.380;95%CI,0.173-0.839; = 0.017),颈内动脉远端受累(OR,0.149;95%CI,0.043-0.520; = 0.003),初始国立卫生研究院卒中量表(NIHSS)评分较低(OR,0.789;95%CI,0.713-0.873; < 0.001),侧支循环良好(OR,13.818;95%CI,3.971-48.090; < 0.001)。多变量分析显示,初始 NIHSS 评分(OR,0.760;95%CI,0.638-0.905; = 0.002)、良好的侧支循环状态(OR,14.130;95%CI,2.264-88.212; = 0.005)和 mTICI 2a 再通(OR,5.636;95%CI,1.216-26.119; = 0.027)仍然是非再通患者良好结局的独立因素。
基线 NIHSS 评分、良好的侧支循环状态和 mTICI 2a 再通与 EVT 后非再通患者的临床结局仍存在独立相关性。mTICI 2a 再通有利于 EVT 后非再通的 AC-LVO 患者中具有良好侧支循环的患者。