Gotland Nanja, Uhre M L, Sandholdt H, Mejer N, Lundbo L F, Petersen A, Larsen A R, Benfield T
Department of Infectious Diseases, Amager Hvidovre Hospital, University of Copenhagen, Hvidovre.
Reference Laboratory for Antimicrobial Resistance and Staphylococci, Statens Serum Institut.
Medicine (Baltimore). 2020 Apr;99(17):e19984. doi: 10.1097/MD.0000000000019984.
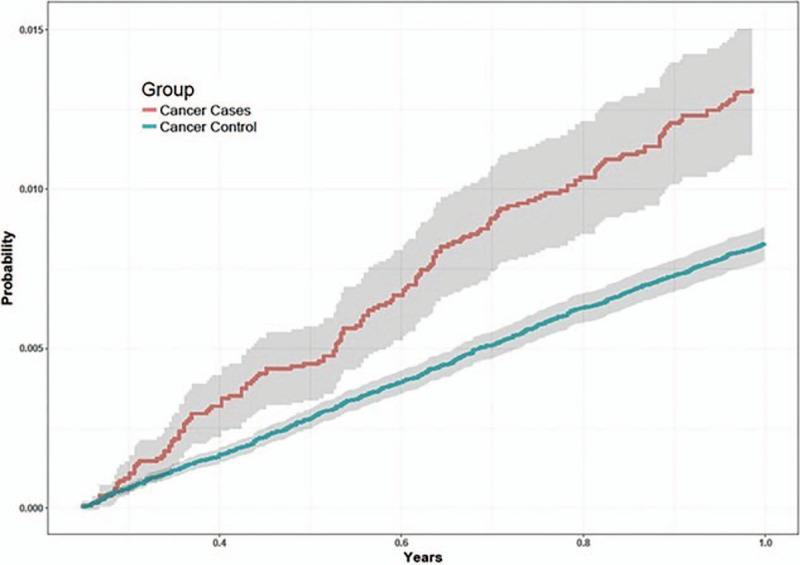
Susceptibility to infectious disease may be a marker of immunodeficiency caused by unrecognized cancer. To test the hypothesis, the risk of incident primary cancer was estimated among survivors of Staphylococcus aureus bacteremia (SAB) and compared to a random population cohort.Nation-wide population-based matched cohort study. Cases of SAB were identified from a national database and incident primary cancers were ascertained by record linkage. Incidence rate (IR) and ratio (IRR) with 95% confidence interval (CI) of 27 cancers was calculated by Poisson regression.During the first year of follow-up, 165 and 943 incident cases of cancer occurred in the case cohort (n = 12,918 (1.3%)) and the population cohort (n = 117,465 (0.8%)) for an IR of 3.78 (3.22-4.40) and 2.28 (2.14-2.43) per 100,000 person-years. The IRR was 1.65 (1.40-1.95). Of 27 cancers, 7 cancers occurred more frequently amongst cases than controls: cervical cancer (IRR 37.83 (4.23-338.47)), multiple myeloma (IRR 6.31 (2.58-15.44)), leukemia (IRR 4.73 (2.21-10.10)), sarcoma (IRR 4.73 (1.18-18.91)), liver cancer (IRR 3.64 (1.30-10.21)), pancreatic cancer (IRR 2.8 (1.27-6.16)), and urinary tract cancer (IRR 2.58 (1.23-5.39)). Compared to the control population, the risk of cancer was higher for those without comorbidity and with younger age. The overall risk of cancer during 2 to 5 years of follow-up was not increased (IRR 0.99 (95% CI: 0.89-1.11). However, the risk of pharyngeal cancer was increased (IRR 1.88 (1.04-3.39)) and the risk of liver cancer remained increased (IRR 3.93 (2.36-6.55)).The risk of primary incident cancer was 65% higher in the SAB cohort compared to the population cohort during the first year of follow-up and included 7 specific cancers. The risk was higher for those without comorbidity and with younger age. Screening for these specific cancers in selected populations may allow for earlier detection.
对传染病的易感性可能是未被识别的癌症所致免疫缺陷的一个标志。为验证这一假设,我们估计了金黄色葡萄球菌菌血症(SAB)幸存者发生原发性癌症的风险,并与随机人群队列进行比较。
全国基于人群的匹配队列研究。通过国家数据库识别SAB病例,并通过记录链接确定原发性癌症的发生情况。采用泊松回归计算27种癌症的发病率(IR)和发病率比(IRR)以及95%置信区间(CI)。
在随访的第一年,病例队列(n = 12,918(1.3%))和人群队列(n = 117,465(0.8%))中分别有165例和943例新发癌症病例,每10万人年的IR分别为3.78(3.22 - 4.40)和2.28(2.14 - 2.43)。IRR为1.65(1.40 - 1.95)。在27种癌症中,有7种癌症在病例组中的发生频率高于对照组:宫颈癌(IRR 37.83(4.23 - 338.47))、多发性骨髓瘤(IRR 6.31(2.58 - 15.44))、白血病(IRR 4.73(2.21 - 10.10))、肉瘤(IRR 4.73(1.18 - 18.91))、肝癌(IRR 3.64(1.30 - 10.21))、胰腺癌(IRR 2.8(1.27 - 6.16))和泌尿系统癌症(IRR 2.58(1.23 - 5.39))。与对照人群相比,无合并症且年龄较小者患癌风险更高。在随访2至5年期间,总体患癌风险未增加(IRR 0.99(95% CI:0.89 - 1.11))。然而,咽喉癌风险增加(IRR 1.88(1.04 - 3.39)),肝癌风险仍然增加(IRR 3.93(2.36 - 6.55))。
在随访的第一年,SAB队列中原发性癌症的风险比人群队列高65%,且包括7种特定癌症。无合并症且年龄较小者风险更高。在特定人群中对这些特定癌症进行筛查可能有助于早期发现。