Department of Pulmonary Circulation, Thromboembolic Diseases and Cardiology, Centre of Postgraduate Medical Education, European Health Centre, Otwock, Poland.
Department of Gerontology, Public Health and Didactics, National Institute of Geriatrics, Rheumatology and Rehabilitation, Warsaw, Poland.
Ann Noninvasive Electrocardiol. 2020 Sep;25(5):e12758. doi: 10.1111/anec.12758. Epub 2020 Apr 26.
The remodeling of the right heart in patients with chronic pulmonary hypertension (cPH) is associated with the appearance of electrocardiographic (ECG) abnormalities. We investigated the resolution of ECG markers of right ventricular hypertrophy (RVH) caused by acute and long-term hemodynamic improvement.
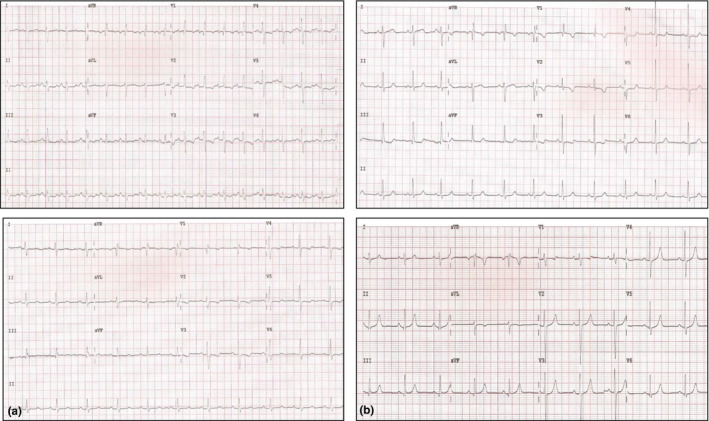
Twenty-nine (29) patients with chronic thromboembolic pulmonary hypertension (CTEPH) and seven patients with pulmonary arterial hypertension (PAH) were included in the analysis. Patients with CTEPH achieved a significant long-term hemodynamic improvement following the treatment with balloon pulmonary angioplasty (BPA); all the patients with PAH reported significant acute hemodynamic relief after a single inhalation of iloprost, fulfilling the criteria of responder. Standard 12-lead ECG was performed before and after intervention.
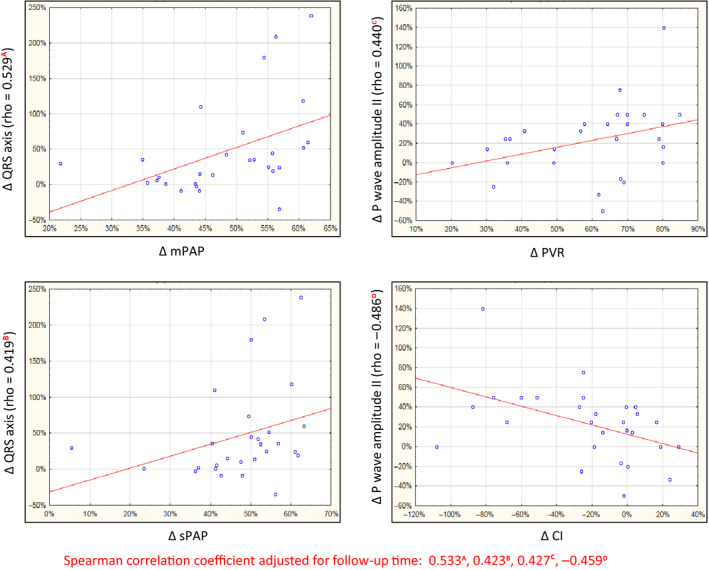
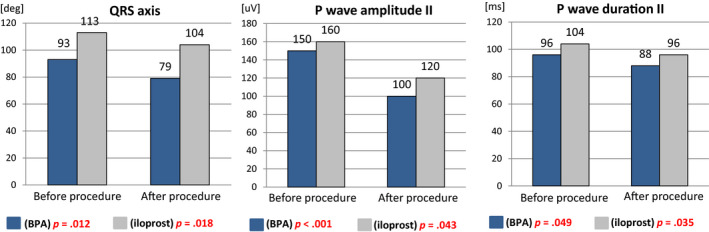
The interval between baseline and control ECG in CTEPH and PAH groups was 28 (IQR: 17-36) months and 15 min (IQR: 11-17), respectively. Despite similar hemodynamic improvement in both groups, only the CTEPH group presented significant changes in most analyzed ECG parameters: T-wave axis (p = .002), QRS-wave axis (p = .012), P-wave amplitude (p < .001) and duration in II (p = .049), R-wave amplitude in V (p = .017), R:S ratio in V (p = .046), S-wave amplitude in V (p = .004), R-wave amplitude in V (p = .044), R:S ratio in V (p = .004), S-wave amplitude in V (p = .026), R-wave amplitude in V (p = .01), and R-wave amplitude in aVR (p = .031). In patients with PAH, significant differences were found only for P wave in II (duration: p = .035; amplitude: p = .043) and QRS axis (p = .018).
The effective treatment of cPH ensures improvement in ECG parameters of RVH, but it requires extended time.
慢性肺动脉高压(cPH)患者的右心重构与心电图(ECG)异常的出现有关。我们研究了急性和长期血流动力学改善引起的右心室肥厚(RVH)的 ECG 标志物的消退情况。
共纳入 29 例慢性血栓栓塞性肺动脉高压(CTEPH)患者和 7 例肺动脉高压(PAH)患者。CTEPH 患者经球囊肺动脉成形术(BPA)治疗后,长期血流动力学显著改善;所有 PAH 患者单次吸入伊洛前列素后,血流动力学均显著缓解,符合应答者标准。在干预前后进行标准 12 导联心电图检查。
CTEPH 和 PAH 组基线和对照心电图之间的间隔分别为 28(IQR:17-36)个月和 15 分钟(IQR:11-17)。尽管两组的血流动力学改善相似,但只有 CTEPH 组的大多数分析的 ECG 参数发生了显著变化:T 波轴(p=0.002)、QRS 波轴(p=0.012)、P 波振幅(p<0.001)和 II 导联的持续时间(p=0.049)、V 导联的 R 波振幅(p=0.017)、V 导联的 R:S 比值(p=0.046)、V 导联的 S 波振幅(p=0.004)、V 导联的 R 波振幅(p=0.044)、V 导联的 R:S 比值(p=0.004)、V 导联的 S 波振幅(p=0.026)、V 导联的 R 波振幅(p=0.01)和 aVR 导联的 R 波振幅(p=0.031)。在 PAH 患者中,仅发现 II 导联的 P 波(持续时间:p=0.035;振幅:p=0.043)和 QRS 轴(p=0.018)有显著差异。
cPH 的有效治疗可改善 RVH 的 ECG 参数,但需要更长的时间。