Bush Andrew
Department of Paediatric Respiratory Medicine, Royal Brompton Hospital Harefield NHS Foundation Trust, Sydney Street, London SW3 6NP, UK.
Paediatric Respiratory Medicine, National Heart and Lung Institute, Imperial College, Sydney Street, London SW3 6NP, UK.
J Fungi (Basel). 2020 Apr 27;6(2):55. doi: 10.3390/jof6020055.
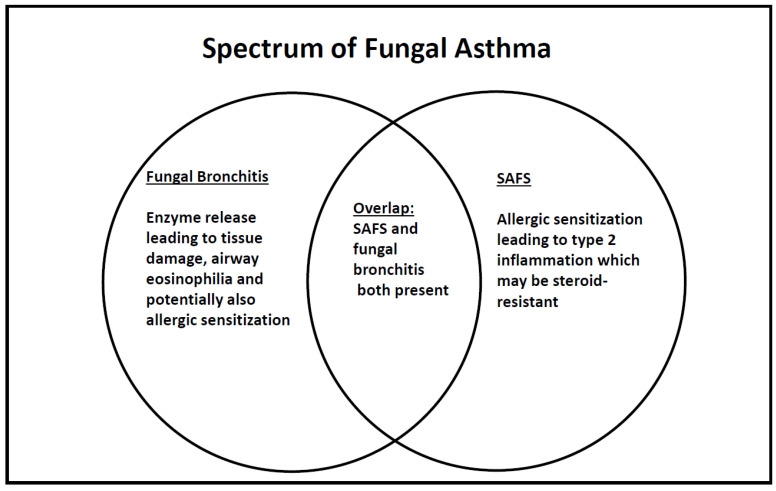
Fungi have many potential roles in paediatric asthma, predominantly by being a source of allergens (severe asthma with fungal sensitization, SAFS), and also directly damaging the epithelial barrier and underlying tissue by releasing proteolytic enzymes (fungal bronchitis). The umbrella term 'fungal asthma' is proposed for these manifestations. Allergic bronchopulmonary aspergillosis (ABPA) is not a feature of childhood asthma, for unclear reasons. Diagnostic criteria for SAFS are based on sensitivity to fungal allergen(s) demonstrated either by skin prick test or specific IgE. In children, there are no exclusion criteria on total IgE levels or IgG precipitins because of the rarity of ABPA. Diagnostic criteria for fungal bronchitis are much less well established. Data in adults and children suggest SAFS is associated with worse asthma control and greater susceptibility to asthma attacks than non-sensitized patients. The data on whether anti-fungal therapy is beneficial are conflicting. The pathophysiology of SAFS is unclear, but the epithelial alarmin interleukin-33 is implicated. However, whether individual fungi have different pathobiologies is unclear. There are many unanswered questions needing further research, including how fungi interact with other allergens, bacteria, and viruses, and what optimal therapy should be, including whether anti-neutrophilic strategies, such as macrolides, should be used. Considerable further research is needed to unravel the complex roles of different fungi in severe asthma.
真菌在儿童哮喘中具有多种潜在作用,主要作为变应原来源(真菌致敏性重度哮喘,SAFS),还可通过释放蛋白水解酶直接破坏上皮屏障及下方组织(真菌性支气管炎)。针对这些表现,提出了“真菌性哮喘”这一统称。过敏性支气管肺曲霉病(ABPA)并非儿童哮喘的特征,原因不明。SAFS的诊断标准基于皮肤点刺试验或特异性IgE证实的对真菌变应原的敏感性。在儿童中,由于ABPA罕见,不存在总IgE水平或IgG沉淀素的排除标准。真菌性支气管炎的诊断标准则远未确立。成人和儿童的数据表明,与未致敏患者相比,SAFS与哮喘控制较差及哮喘发作易感性较高有关。关于抗真菌治疗是否有益的数据相互矛盾。SAFS的病理生理学尚不清楚,但上皮警报素白细胞介素-33与之有关。然而,个体真菌是否具有不同的病理生物学尚不清楚。有许多未解决的问题需要进一步研究,包括真菌如何与其他变应原、细菌和病毒相互作用,以及最佳治疗方案应该是什么,包括是否应使用抗中性粒细胞策略,如大环内酯类药物。需要进行大量进一步研究以阐明不同真菌在重度哮喘中的复杂作用。