Thoracic Oncology Service, Division of Solid Tumor Oncology, Department of Medicine, Memorial Sloan Kettering Cancer Center, Weill Cornell Medical College, New York, New York, United States.
Department of Radiation Oncology, Memorial Sloan Kettering Cancer Center, New York, New York, United States.
Radiother Oncol. 2020 Aug;149:205-211. doi: 10.1016/j.radonc.2020.04.047. Epub 2020 Apr 30.
Concurrent chemoradiation (cCRT) and durvalumab is standard therapy for patients with unresectable stage III non-small-cell lung cancers (NSCLC). Data is limited on outcomes with this regimen outside of clinical trials. Local-regional control rates remain undefined.
We reviewed patients with stage III unresectable NSCLCs treated between November 2017 and February 2019 with cCRT and ≥1 dose of durvalumab. We examined 12-month progression-free-survival (PFS), overall-survival (OS), toxicities, and the incidence and pattern of local-regional and metastatic failures.
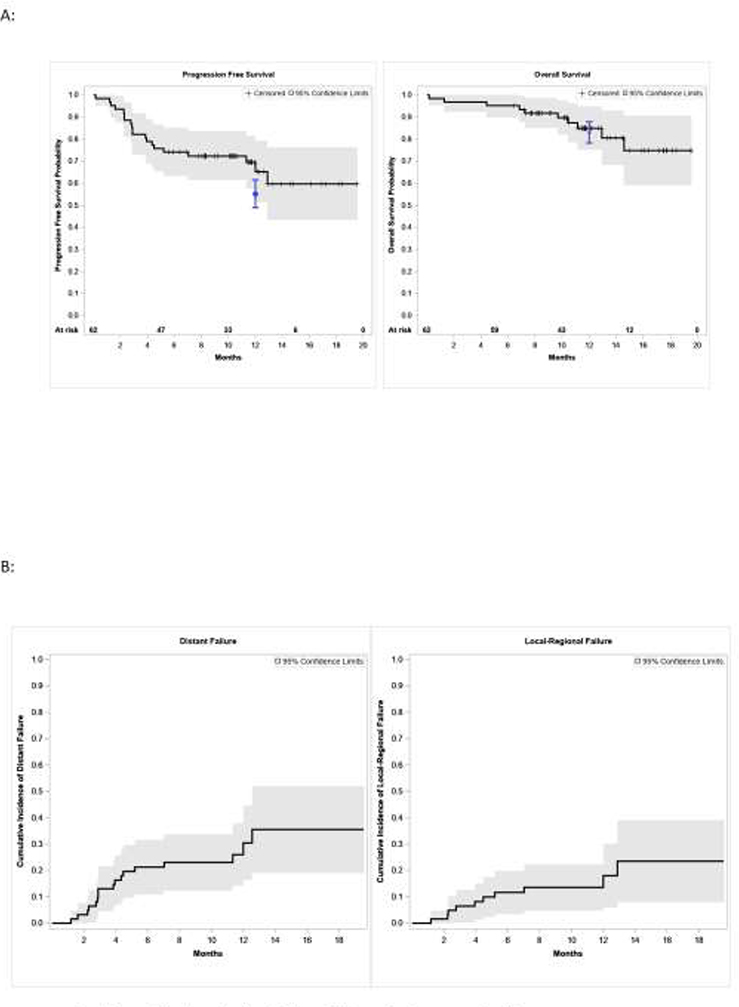
Sixty-two patients (median follow-up 12 months) with median age of 66 years of which 73% had stage IIIB (n = 33) or IIIC (n = 12) disease started durvalumab a median of 1.5 months from the end of cCRT and were treated with a median of 8 months of durvalumab. Common reasons for stopping durvalumab included disease progression (32%, 20/62) and toxicity (24%, 15/62). The estimated 12-month PFS and OS were 65% (95% CI: 51-79%) and 85% (95% CI: 75-95%), respectively. The cumulative 12-month incidence of local-regional and distant failures were 18% (95% CI: 5.9-30%) and 30% (95% CI: 16.3-44.5%), respectively. Among patients with distant metastatic disease (n = 17), 47% had oligometastatic disease. High tumor mutation burden (≥8.8 mt/Mb) or PD-L1 (≥1% or PD-L1 ≥ 50%) did not predict improved PFS.
Outcomes with cCRT and durvalumab in practice align with the PACIFIC trial. A substantial minority of patients are candidates for metastasis-directed therapies at progression. Local regional outcomes appear improved to historical data of cCRT alone.
同期放化疗(cCRT)联合度伐利尤单抗是不可切除 III 期非小细胞肺癌(NSCLC)患者的标准治疗方法。该方案在临床试验之外的数据有限。局部区域控制率尚未确定。
我们回顾了 2017 年 11 月至 2019 年 2 月期间接受 cCRT 和至少 1 剂度伐利尤单抗治疗的不可切除 III 期 NSCLC 患者。我们检查了 12 个月无进展生存期(PFS)、总生存期(OS)、毒性反应,以及局部区域和转移性失败的发生率和模式。
62 例患者(中位随访时间 12 个月),中位年龄为 66 岁,其中 73%(n=33)为 IIIB 期或 IIIC 期(n=12)疾病,在 cCRT 结束后中位 1.5 个月开始接受度伐利尤单抗治疗,中位治疗时间为 8 个月。停止度伐利尤单抗治疗的常见原因包括疾病进展(32%,20/62)和毒性(24%,15/62)。估计的 12 个月 PFS 和 OS 分别为 65%(95%CI:51-79%)和 85%(95%CI:75-95%)。12 个月时局部区域和远处失败的累积发生率分别为 18%(95%CI:5.9-30%)和 30%(95%CI:16.3-44.5%)。在远处转移疾病患者(n=17)中,47%患者存在寡转移疾病。高肿瘤突变负荷(≥8.8 mt/Mb)或 PD-L1(≥1%或 PD-L1≥50%)并不能预测 PFS 的改善。
cCRT 联合度伐利尤单抗的实际结果与 PACIFIC 试验一致。相当一部分患者在进展时可接受针对转移的治疗。局部区域结果似乎优于单独接受 cCRT 的历史数据。