Department of Pediatrics, The Johns Hopkins University School of Medicine, Baltimore, Maryland.
Department of Pharmacy, The Johns Hopkins Hospital, Baltimore, Maryland.
JAMA Netw Open. 2020 May 1;3(5):e203951. doi: 10.1001/jamanetworkopen.2020.3951.
National guidelines recommend treating children with pyelonephritis for 7 to 14 days of antibiotic therapy, yet data are lacking to suggest a more precise treatment duration.
To compare the clinical outcomes of children receiving a short-course vs a prolonged-course of antibiotic treatment for pyelonephritis.
DESIGN, SETTING, AND PARTICIPANTS: Retrospective observational study using inverse probability of treatment weighted propensity score analysis of data from 5 hospitals in Maryland between July 1, 2016, and October 1, 2018. Participants were children aged 6 months to 18 years with a urine culture growing Escherichia coli, Klebsiella species, or Proteus mirabilis with laboratory and clinical criteria for pyelonephritis.
Treatment of pyelonephritis with a short-course (6 to 9 days) vs a prolonged-course (10 or more days) of antibiotics.
Composite outcome of treatment failure within 30 days of completing antibiotic therapy: (a) unanticipated emergency department or outpatient visits related to urinary tract infection symptoms, (b) hospital readmission related to UTI symptoms, (c) prolongation of the planned, initial antibiotic treatment course, or (d) death. A subsequent urinary tract infection caused by a drug-resistant bacteria within 30 days was a secondary outcome.
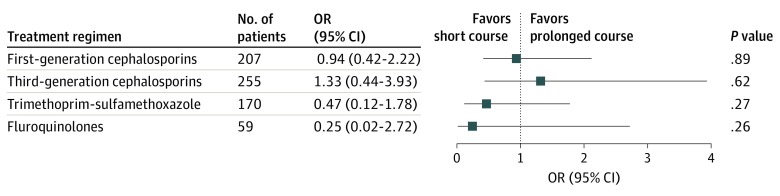
Of 791 children who met study eligibility criteria (mean [SD] age 9.2 [6.3] years; 672 [85.0%]) were girls, 297 patients (37.5%) were prescribed a short-course and 494 patients (62.5%) were prescribed a prolonged-course of antibiotics. The median duration of short-course therapy was 8 days (interquartile range, 7-8 days), and the median duration of prolonged-course therapy was 11 days (interquartile range, 11-12 days). Baseline characteristics were similar between the groups in the inverse probability of treatment weighted cohort. There were 79 children (10.1%) who experienced treatment failure. The odds of treatment failure were similar for patients prescribed a short-course vs a prolonged-course of antibiotics (11.2% vs 9.4%; odds ratio, 1.22; 95% CI, 0.75-1.98). There was no significant difference in the odds of a drug-resistant uropathogen for patients with a subsequent urinary tract infection within 30 days when prescribed a short-courses vs prolonged-course of antibiotics (40% vs 64%; odds ratio, 0.36; 95% CI, 0.09-1.43).
The study findings suggest that short-course antibiotic therapy may be as effective as prolonged-courses for children with pyelonephritis, and may mitigate the risk of future drug-resistant urinary tract infections. Additional studies are needed to confirm these findings.
国家指南建议对患有肾盂肾炎的儿童进行 7 至 14 天的抗生素治疗,但缺乏数据表明更精确的治疗持续时间。
比较接受短期和延长疗程抗生素治疗肾盂肾炎的儿童的临床结局。
设计、地点和参与者:2016 年 7 月 1 日至 2018 年 10 月 1 日期间,马里兰州 5 家医院的回顾性观察性研究。参与者为年龄在 6 个月至 18 岁之间、尿液培养出大肠埃希菌、克雷伯氏菌属或奇异变形杆菌且有实验室和临床标准的肾盂肾炎的儿童。
用短疗程(6 至 9 天)和长疗程(10 天或以上)抗生素治疗肾盂肾炎。
在完成抗生素治疗后 30 天内治疗失败的综合结果:(a)与尿路感染症状相关的意外急诊就诊或门诊就诊,(b)因 UTI 症状再次住院,(c)延长计划的初始抗生素治疗疗程,或(d)死亡。30 天内由耐药细菌引起的继发尿路感染为次要结果。
符合研究条件的 791 名儿童(平均[SD]年龄 9.2[6.3]岁;672[85.0%] 名女孩)中,297 名患者(37.5%)接受了短疗程治疗,494 名患者(62.5%)接受了长疗程治疗。短疗程治疗的中位持续时间为 8 天(四分位距,7-8 天),长疗程治疗的中位持续时间为 11 天(四分位距,11-12 天)。在反概率治疗加权队列中,两组的基线特征相似。79 名儿童(10.1%)发生治疗失败。接受短疗程和长疗程抗生素治疗的儿童治疗失败的几率相似(11.2%比 9.4%;比值比,1.22;95%CI,0.75-1.98)。在 30 天内发生继发尿路感染的患者中,使用短疗程和长疗程抗生素治疗的药物耐药尿路病原体的几率没有显著差异(40%比 64%;比值比,0.36;95%CI,0.09-1.43)。
研究结果表明,对于患有肾盂肾炎的儿童,短疗程抗生素治疗可能与长疗程一样有效,并可能降低未来发生耐药性尿路感染的风险。需要进一步的研究来证实这些发现。