Department of Surgery, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia.
Department of Surgery, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand.
Cancer Med. 2020 Jul;9(13):4613-4621. doi: 10.1002/cam4.3101. Epub 2020 May 6.
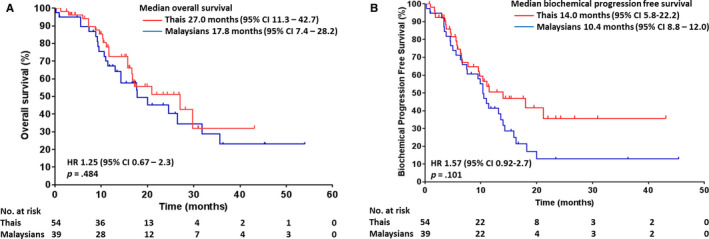
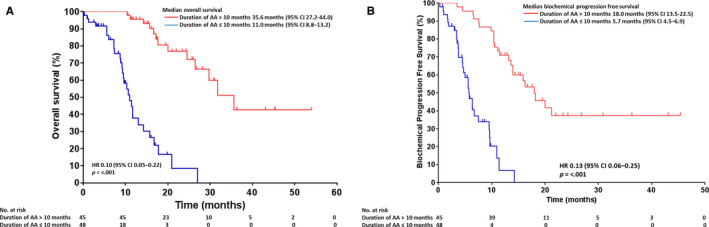
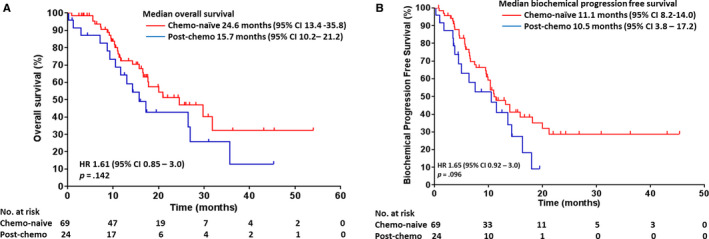
It is of much interest to understand the efficacy of abiraterone acetate (AA) in routine clinical practice. We assessed the clinical outcome of AA in patients with metastatic castration-resistant prostate cancer (mCRPC) and determined clinical factors associated with AA treatment duration in real-world setting. This real-world cohort consisted of 93 patients with mCRPC treated with AA in Thailand (58.1%) and Malaysia (41.9%). Primary endpoints were overall survival (OS) and biochemical progression-free survival (bPFS). Secondary endpoints were predictors associated with AA treatment duration evaluated with Cox proportional hazards regression. Around 74% were chemotherapy-naïve. The median AA treatment duration was 10 months (IQR 5.6-17.1). Malaysians had a relatively lower median OS and bPFS (OS 17.8 months; 95% CI 6.4-29.1, bPFS 10.4 months; 95% CI 8.8-12.0) compared to Thais (OS 27.0 months; 95% CI 11.3-42.7, bPFS 14.0 months; 95% CI 5.8-22.2), although it did not achieve statistical significance (P > .05). Patients with longer AA treatment duration (>10 months) had lower risk of death and longer bPFS, compared to those with shorter AA treatment duration (≤10 months) (hazard ratio [HR] 0.10, 95% CI 0.05-0.22 and HR 0.13, 95% CI 0.06-0.25, respectively). Multivariable analysis showed that PSA at AA initiation, presence of PSA response and chemotherapy-naive were independently associated with AA duration (P < .05). Abiraterone acetate is well-tolerated in the Southeast Asian cohort with comparable survival benefits to other Asian populations in real-world setting. Lower PSA levels at AA initiation, presence of PSA response, and chemotherapy-naive were significant in determining AA treatment duration.
了解醋酸阿比特龙(AA)在常规临床实践中的疗效很有意义。我们评估了 AA 在转移性去势抵抗性前列腺癌(mCRPC)患者中的临床疗效,并确定了真实世界环境中与 AA 治疗持续时间相关的临床因素。这个真实世界的队列包括 93 名在泰国(58.1%)和马来西亚(41.9%)接受 AA 治疗的 mCRPC 患者。主要终点是总生存期(OS)和生化无进展生存期(bPFS)。次要终点是用 Cox 比例风险回归评估与 AA 治疗持续时间相关的预测因素。约 74%的患者为化疗初治。AA 治疗的中位持续时间为 10 个月(IQR 5.6-17.1)。与泰国人相比,马来西亚人的中位 OS 和 bPFS 相对较低(OS 17.8 个月;95%CI 6.4-29.1,bPFS 10.4 个月;95%CI 8.8-12.0)(OS 27.0 个月;95%CI 11.3-42.7,bPFS 14.0 个月;95%CI 5.8-22.2),尽管这并没有达到统计学意义(P>.05)。与治疗时间较短(≤10 个月)的患者相比,AA 治疗时间较长(>10 个月)的患者死亡风险和 bPFS 更长(风险比[HR]0.10,95%CI 0.05-0.22 和 HR 0.13,95%CI 0.06-0.25)。多变量分析显示,AA 起始时 PSA、PSA 反应的存在和化疗初治与 AA 持续时间独立相关(P<.05)。醋酸阿比特龙在东南亚队列中具有良好的耐受性,在真实世界环境中与其他亚洲人群的生存获益相当。AA 起始时 PSA 水平较低、PSA 有反应以及化疗初治是确定 AA 治疗持续时间的重要因素。