Division of Emergency Medicine, Ann & Robert H. Lurie Children's Hospital, Chicago, Illinois.
Division of Analytics, Children's Hospital Association, Lenexa, Kansas.
JAMA Netw Open. 2020 May 1;3(5):e204185. doi: 10.1001/jamanetworkopen.2020.4185.
Urgent care (UC) centers are a growing option to address children's acute care needs, which may cause unanticipated changes in health care use.
To identify factors associated with high UC reliance among children enrolled in Medicaid and examine the association between UC reliance and outpatient health care use.
DESIGN, SETTING, AND PARTICIPANTS: A retrospective cohort study used deidentified data on 4 133 238 children from the Marketscan Medicaid multistate claims database to calculate UC reliance and outpatient health care use. Children were younger than 19 years, with 11 months or more of continuous Medicaid enrollment and 1 or more UC, emergency department (ED), primary care provider (PCP; physician, advanced practice nurse, or physician assistant; well-child care [WCC] or non-WCC), or specialist outpatient visit during the 2017 calendar year. Statistical analysis was conducted from November 11 to 26, 2019.
Urgent care, ED, PCP (WCC and non-WCC), and specialist visits based on coded location of services.
Urgent care reliance, calculated by the number of UC visits divided by the sum of total outpatient (UC, ED, PCP, and specialist) visits. High UC reliance was defined as UC visits totaling more than 33% of all outpatient visits.
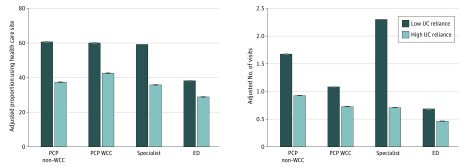
Of 4 133 238 children in the study, 2 090 278 (50.6%) were male, with a median age of 9 years (interquartile range, 4-13 years). A total of 223 239 children (5.4%) had high UC reliance. Children 6 to 12 years of age were more likely to have high UC reliance compared with children 13 to 18 years of age (adjusted odds ratio, 1.07; 95% CI, 1.06-1.09). Compared with white children, black children (adjusted odds ratio, 0.81; 95% CI, 0.81-0.82) and Hispanic children (adjusted odds ratio, 0.61; 95% CI, 0.60-0.61) were less likely to have high UC reliance. Adjusted for age, sex, race/ethnicity, and presence of chronic or complex conditions, children with high UC reliance had significantly fewer PCP encounters (WCC: adjusted rate ratio, 0.60; 95% CI, 0.60-0.61; and non-WCC: adjusted rate ratio, 0.41; 95% CI, 0.41-0.41), specialist encounters (adjusted rate ratio, 0.31; 95% CI, 0.31-0.31), and ED encounters (adjusted rate ratio, 0.68; 95% CI, 0.67-0.68) than children with low UC reliance.
High UC reliance occurred more often in healthy, nonminority, school-aged children and was associated with lower health care use across other outpatient settings. There may be an opportunity in certain populations to ensure that UC reliance does not disrupt the medical home model.
急诊所(UC)中心是满足儿童急性护理需求的一种日益流行的选择,这可能会导致医疗保健使用的意外变化。
确定与参加医疗补助计划的儿童中高度依赖 UC 相关的因素,并检查 UC 依赖与门诊医疗保健使用之间的关联。
设计、地点和参与者: 使用来自 Marketscan 医疗补助多州索赔数据库的 4133238 名儿童的匿名数据进行回顾性队列研究,以计算 UC 依赖和门诊医疗保健使用情况。儿童年龄小于 19 岁,连续参加医疗补助计划 11 个月或以上,在 2017 年日历年内有 1 次或多次 UC、急诊部(ED)、初级保健提供者(PCP;医生、高级执业护士或医师助理;WCC 或非 WCC 保健)或专科门诊就诊。统计分析于 2019 年 11 月 11 日至 26 日进行。
根据服务地点的编码,基于 UC、ED、PCP(WCC 和非 WCC)和专科就诊的 UC 依赖。高 UC 依赖定义为 UC 就诊次数占所有门诊就诊次数(UC、ED、PCP 和专科)的 33%以上。
UC 依赖率,通过 UC 就诊次数除以总门诊(UC、ED、PCP 和专科)就诊次数计算得出。高 UC 依赖率定义为 UC 就诊次数占所有门诊就诊次数的 33%以上。
在研究的 4133238 名儿童中,2090278 名(50.6%)为男性,中位年龄为 9 岁(四分位距,4-13 岁)。共有 223239 名儿童(5.4%)存在高 UC 依赖。与 13 至 18 岁的儿童相比,6 至 12 岁的儿童更有可能出现高 UC 依赖(调整后的优势比,1.07;95%CI,1.06-1.09)。与白人儿童相比,黑人儿童(调整后的优势比,0.81;95%CI,0.81-0.82)和西班牙裔儿童(调整后的优势比,0.61;95%CI,0.60-0.61)不太可能出现高 UC 依赖。调整年龄、性别、种族/民族和存在慢性或复杂疾病后,高 UC 依赖的儿童 PCP 就诊次数明显减少(WCC:调整后率比,0.60;95%CI,0.60-0.61;非 WCC:调整后率比,0.41;95%CI,0.41-0.41)、专科就诊次数(调整后率比,0.31;95%CI,0.31-0.31)和 ED 就诊次数(调整后率比,0.68;95%CI,0.67-0.68)低于 UC 依赖程度低的儿童。
高 UC 依赖在健康、非少数民族、学龄儿童中更为常见,并且与其他门诊就诊环境中的医疗保健使用率降低有关。在某些人群中,可能有机会确保 UC 依赖不会破坏医疗之家模式。