British Columbia Centre for Disease Control, Vancouver, Canada.
Canadian Network on Hepatitis C, Montreal, Quebec, Canada.
JAMA Netw Open. 2020 May 1;3(5):e204192. doi: 10.1001/jamanetworkopen.2020.4192.
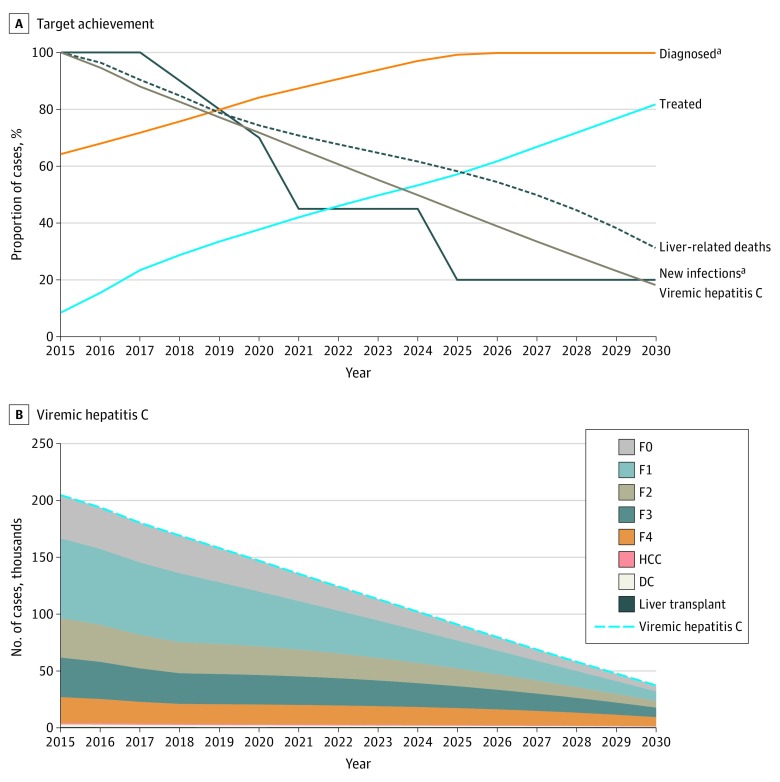
Achievement of the World Health Organization (WHO) target of eliminating hepatitis C virus (HCV) by 2030 will require an increase in key services, including harm reduction, HCV screening, and HCV treatment initiatives in member countries. These data are not available for Canada but are important for informing a national HCV elimination strategy.
To use a decision analytical model to explore the association of different treatment strategies with HCV epidemiology and HCV-associated mortality in Canada and to assess the levels of service increase needed to meet the WHO elimination targets by 2030.
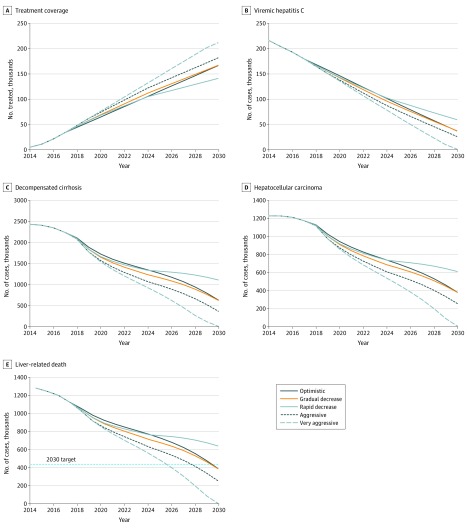
DESIGN, SETTING, AND PARTICIPANTS: Study participants in this decision analytical model included individuals with hepatitis C virus infection in Canada. Five HCV treatment scenarios (optimistic, very aggressive, aggressive, gradual decrease, and rapid decrease) were applied using a previously validated Markov-type mathematical model. The optimistic and very aggressive treatment scenarios modeled a sustained annual treatment of 10 200 persons and 14 000 persons, respectively, from 2018 to 2030. The aggressive, gradual decrease, and rapid decrease scenarios assessed decreases in treatment uptake from 14 000 persons to 10 000 persons per year, 12 000 persons to 8500 persons per year, and 12 000 persons to 4500 persons per year, respectively, between 2018 and 2030.
Hepatitis C virus prevalence and HCV-associated health outcomes were assessed for each of the 5 treatment scenarios with the goal of identifying strategies to achieve HCV elimination by 2030.
An estimated mean 180 142 persons (95% CI, 122 786-196 862 persons) in Canada had chronic HCV infection at the end of 2017. The optimistic and gradual decrease scenarios estimated a decrease in HCV prevalence from 180 142 persons to 37 246 persons and 37 721 persons, respectively, by 2030. Relative to 2015, this decrease in HCV prevalence was associated with 74%, 69%, and 69% reductions in the prevalence of decompensated cirrhosis, hepatocellular carcinoma, and liver-associated mortality, respectively, leading to HCV elimination by 2030. More aggressive treatment uptake (very aggressive scenario) could result in goal achievement up to 3 years earlier than 2030, although a rapid decrease in the initiation of treatment (rapid decrease scenario) would preclude Canada from reaching the HCV elimination goal by 2030.
The study findings suggest that Canada could meet the WHO goals for HCV elimination by 2030 by sustaining the current national HCV treatment rate during the next decade. This target will not be achieved if treatment uptake is allowed to decrease rapidly.
到 2030 年实现世界卫生组织(WHO)消除丙型肝炎病毒(HCV)的目标,需要在会员国中增加关键服务,包括减少伤害、HCV 筛查和 HCV 治疗措施。加拿大没有这些数据,但对于制定国家 HCV 消除战略很重要。
使用决策分析模型探讨不同治疗策略与加拿大 HCV 流行病学和 HCV 相关死亡率的关系,并评估到 2030 年达到世卫组织消除目标所需的服务水平增加。
设计、设置和参与者:本决策分析模型的研究参与者包括加拿大 HCV 感染者。采用先前验证的马尔可夫型数学模型,对五种 HCV 治疗方案(乐观、非常积极、积极、逐渐减少和快速减少)进行了应用。乐观和非常积极的治疗方案分别模拟 2018 年至 2030 年期间每年持续治疗 10200 人和 14000 人。积极、逐渐减少和快速减少方案分别评估了从 2018 年至 2030 年期间每年治疗人数从 14000 人减少到 10000 人、从 14000 人减少到 8500 人以及从 12000 人减少到 4500 人。
对五种治疗方案中的每一种方案进行 HCV 流行率和 HCV 相关健康结果评估,目的是确定到 2030 年实现 HCV 消除的策略。
2017 年底,加拿大估计有 180142 人(95%CI,122786-196862 人)患有慢性 HCV 感染。乐观和逐渐减少的方案预计到 2030 年,HCV 流行率将从 180142 人下降到 37246 人和 37721 人。与 2015 年相比,这种 HCV 流行率的下降与失代偿性肝硬化、肝细胞癌和与肝脏相关的死亡率的患病率分别降低 74%、69%和 69%有关,从而到 2030 年实现 HCV 消除。更积极的治疗采用(非常积极的方案)可能会导致提前 3 年实现目标,尽管治疗开始的快速减少(快速减少方案)将使加拿大无法到 2030 年实现 HCV 消除目标。
研究结果表明,加拿大可以在未来十年内维持目前的全国 HCV 治疗率,以实现到 2030 年世卫组织消除 HCV 的目标。如果治疗采用率允许迅速下降,则无法实现这一目标。