Obstetrics and Gynecology, University of Southern California, Los Angeles, California, USA
Division of Gynecologic Oncology, Department of Obstetrics and Gynecology, University of Southern California, Los Angeles, California, USA.
Int J Gynecol Cancer. 2020 Sep;30(9):1331-1339. doi: 10.1136/ijgc-2020-001362. Epub 2020 May 5.
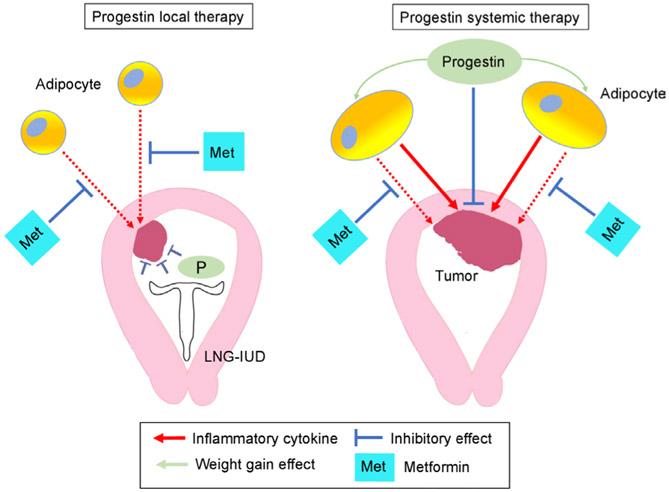
Previous studies have suggested that metformin use may enhance the therapeutic effect of progestin therapy for endometrial hyperplasia or malignancy. However, it is not known how the impact of concurrent metformin may be altered by route of progestin therapy, either locally via an intrauterine device or systemically. This study examined the effectiveness of concurrent metformin use and progestin therapy for women with complex atypical hyperplasia stratified by progestin route (systemic vs local).
This single-institution retrospective study examined consecutive women with complex atypical hyperplasia who received progestin therapy from 2003 to 2018. Time-dependent analyses for complete response rate were performed comparing concurrent metformin users versus non-users in the oral progestin group and in the levonorgestrel-releasing intrauterine device group.
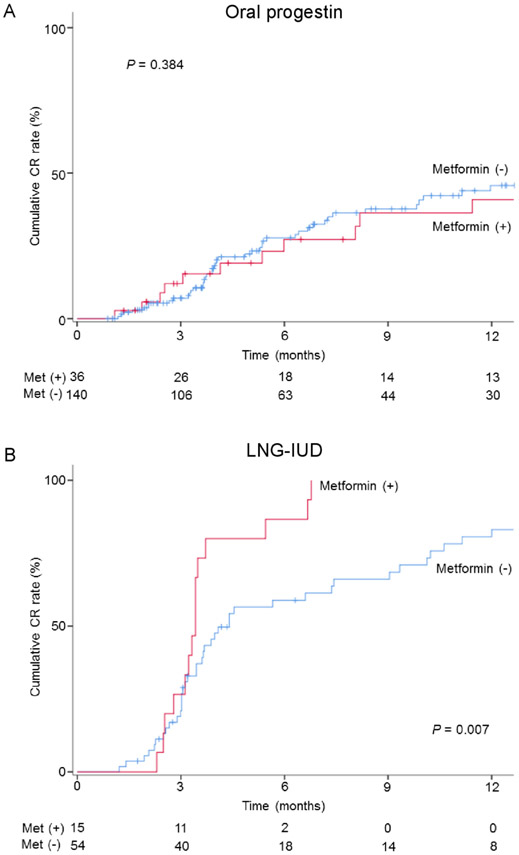
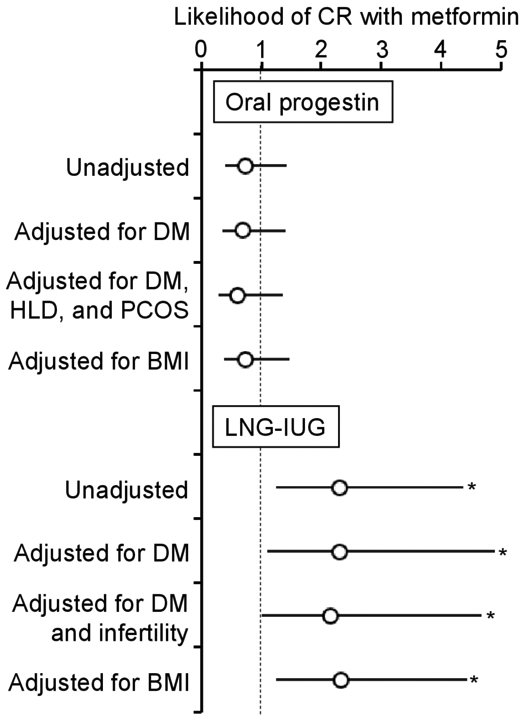
Across the study cohort (n=245), there were 137 (55.9%) women who responded to progestin therapy. In the oral progestin group (n=176), the median age and body mass index were 36 years and 37.7 kg/m, respectively. 36 (20.5%) of women on oral progestins also took metformin. After controlling for diabetes status, women taking both oral progestins and metformin had a complete response rate similar to those not taking metformin (6 month cumulative rates, 23.1% vs 27.8%, adjusted hazard ratio (aHR) 0.71, 95% confidence interval (95% CI) 0.36 to 1.41). In the levonorgestrel-releasing intrauterine device group (n=69), the median age and body mass index were 35 years and 39.9 kg/m, respectively. There were 15 (21.7%) women who took metformin in addition to the levonorgestrel-releasing intrauterine device. After controlling for diabetes status, women who had the levonorgestrel-releasing intrauterine device and took metformin had a significantly higher complete response rate compared with those not taking metformin (6 month cumulative rates, 86.7% vs 58.9%, aHR 2.31, 95% CI 1.09 to 4.89).
In a predominantly obese population, concurrent metformin may possibly offer treatment benefit when used with the levonorgestrel-releasing intrauterine device.
先前的研究表明,二甲双胍的使用可能会增强孕激素治疗子宫内膜增生或恶性肿瘤的疗效。然而,目前尚不清楚孕激素治疗途径(局部通过宫内节育器或全身)如何改变同时使用二甲双胍的影响。本研究通过孕激素途径(全身与局部)分层,检查同时使用二甲双胍和孕激素治疗患有复杂性非典型增生的妇女的效果。
本单中心回顾性研究检查了 2003 年至 2018 年期间接受孕激素治疗的复杂性非典型增生的连续女性。在口服孕激素组和左炔诺孕酮宫内节育器组中,对同时使用二甲双胍与未使用者的完全缓解率进行了时间依赖性分析。
在整个研究队列(n=245)中,有 137(55.9%)名妇女对孕激素治疗有反应。在口服孕激素组(n=176)中,中位年龄和体重指数分别为 36 岁和 37.7kg/m。36(20.5%)名口服孕激素的妇女也服用二甲双胍。在控制糖尿病状态后,同时服用口服孕激素和二甲双胍的妇女的完全缓解率与未服用二甲双胍的妇女相似(6 个月累积率,23.1%对 27.8%,调整后的危险比(aHR)0.71,95%置信区间(95%CI)0.36 至 1.41)。在左炔诺孕酮宫内节育器组(n=69)中,中位年龄和体重指数分别为 35 岁和 39.9kg/m。除左炔诺孕酮宫内节育器外,还有 15(21.7%)名妇女服用二甲双胍。在控制糖尿病状态后,同时使用左炔诺孕酮宫内节育器和二甲双胍的妇女的完全缓解率明显高于未服用二甲双胍的妇女(6 个月累积率,86.7%对 58.9%,aHR 2.31,95%CI 1.09 至 4.89)。
在以肥胖为主的人群中,同时使用二甲双胍可能会与左炔诺孕酮宫内节育器一起带来治疗益处。