Health Research, Res Consortium, Andover, UK.
ARC Epidemiology Unit, University of Manchester, Manchester, UK.
BMJ Open. 2020 May 5;10(5):e033231. doi: 10.1136/bmjopen-2019-033231.
Other than age, diabetes is the largest contributor to overall healthcare costs and reduced life expectancy in Europe. This paper aims to more exactly quantify the net impact of diabetes on different aspects of healthcare provision in hospitals in England, building on previous work that looked at the determinants of outcome in type 1 diabetes (T1DM) and type 2 diabetes (T2DM).
NHS Digital Hospital Episode Statistics (HES) in England was combined with the National Diabetes Audit (NDA) to provide the total number in practice of people with T1DM/T2DM.
We compared differences between T1DM/T2DM and non-diabetes individuals in relation to hospital activity and associated cost.
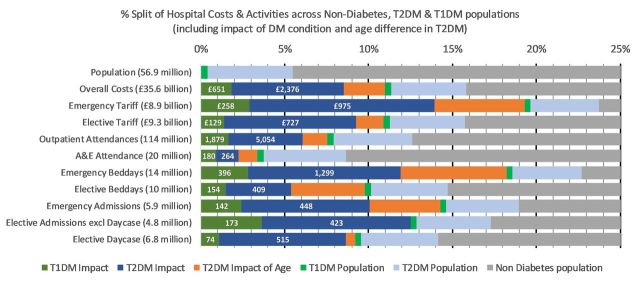
The study captured 90% of hospital activity and £36 billion/year of hospital spend. The NDA Register showed that out of a total reported population of 58 million, 2.9 million (6.5%) had T2DM and 240 000 (0.6%) had T1DM. Bed-day analysis showed 17% of beds are occupied by T2DM and 3% by T1DM. The overall cost of hospital care for people with diabetes is £5.5 billion/year. Once the normally expected costs including the older age of T2DM hospital attenders are allowed for this fell to £3.0 billion/year or 8% of the total captured secondary care costs. This equates to £560/non-diabetes person compared with £3280/person with T1DM and £1686/person with T2DM. For people with diabetes, the net excess impact on non-elective/emergency work is £1.2 billion with additional estimated diabetes-related accident & emergency attendances at 440 000 costing the NHS £70 million/year. T1DM individuals required five times more secondary care support than non-diabetes individuals. T2DM individuals, even allowing for the age, require twice as much support as non-diabetes individuals.
This analysis shows that additional cost of provision of hospital services due to their diabetes comorbidities is £3 billion above that for non-diabetes, and that within this, T1DM has three times as much cost impact as T2DM. We suggest that supporting patients in diabetes management may significantly reduce hospital activity.
除年龄外,糖尿病是导致欧洲医疗保健费用整体增加和预期寿命降低的最大因素。本文旨在在前瞻性研究 1 型糖尿病(T1DM)和 2 型糖尿病(T2DM)结局决定因素的基础上,更准确地量化糖尿病对英国医院提供医疗服务的各个方面的净影响。
英格兰国民保健署(NHS)数字医院病例统计(HES)与国家糖尿病审计(NDA)相结合,提供 T1DM/T2DM 患者的实际人数。
我们比较了 T1DM/T2DM 患者与非糖尿病患者在医院活动和相关费用方面的差异。
该研究涵盖了 90%的医院活动和 360 亿英镑/年的医院支出。NDA 登记册显示,在报告的 5800 万总人口中,290 万人(6.5%)患有 T2DM,24 万人(0.6%)患有 T1DM。床位分析显示,2 型糖尿病患者占用床位的 17%,1 型糖尿病患者占用床位的 3%。糖尿病患者的医院总护理费用为 55 亿英镑/年。一旦考虑到 2 型糖尿病住院患者年龄较大的正常预期成本,这一数字降至 30 亿英镑/年,占捕获的二级护理总成本的 8%。这相当于每非糖尿病患者 560 英镑,每 1 型糖尿病患者 3280 英镑,每 2 型糖尿病患者 1686 英镑。对于糖尿病患者,非选择性/紧急治疗工作的净额外影响为 12 亿英镑,额外估计糖尿病相关的急诊就诊人数为 44 万,每年 NHS 花费 7000 万英镑。T1DM 患者所需的二级护理支持是非糖尿病患者的五倍。即使考虑到年龄,T2DM 患者的护理需求也是非糖尿病患者的两倍。
这项分析表明,由于糖尿病合并症,医院服务提供的额外费用比非糖尿病患者高出 30 亿英镑,而在这其中,T1DM 的成本影响是 T2DM 的三倍。我们建议,通过支持糖尿病患者的管理,可能会显著减少医院活动。