Department of Anaesthesiology, Medical Faculty, RWTH Aachen University, Pauwelsstr. 30, 52074, Aachen, Germany.
Department of Anaesthesiology and Critical Care Medicine, Faculty of Medicine, University Hospital Freiburg, Freiburg, Germany.
Anaesthesist. 2021 Dec;70(Suppl 1):38-47. doi: 10.1007/s00101-020-00773-y. Epub 2020 Jul 6.
In 2016 the German Society of Anesthesiology and Intensive Care Medicine (DGAI) and the Association of German Anesthetists (BDA) published 10 quality indicators (QI) to compare and improve the quality of anesthesia care in Germany. So far, there is no evidence for the feasibility of implementation of these QI in hospitals.
This study tested the hypothesis that the implementation of the 10 QI is feasible in German hospitals.
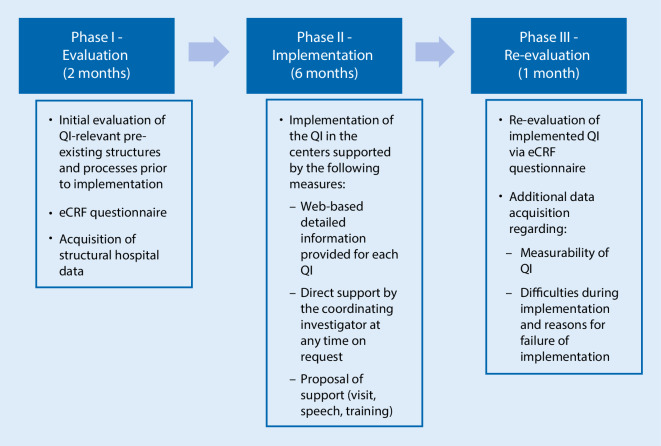
This prospective three-phase national multicenter quality improvement study was conducted in 15 German hospitals and 1 outpatient anesthesia center from March 2017 to February 2018. The trial consisted of an initial evaluation of pre-existing structures and processes by the heads of the participating anesthesia departments, followed by a 6-month implementation phase of the QI as well as a final re-evaluation phase. The implementation procedure was supported by web-based implementation aids ( www.qi-an.org ) and internal quality management programs. The primary endpoint was the difference in the number of implemented QI per center before and after implementation. Secondary endpoints were the number of newly implemented QI per center, the overall number of successful implementations of each QI, the identification of problems during the implementation as well as the kind of impediments preventing the QI implementation.
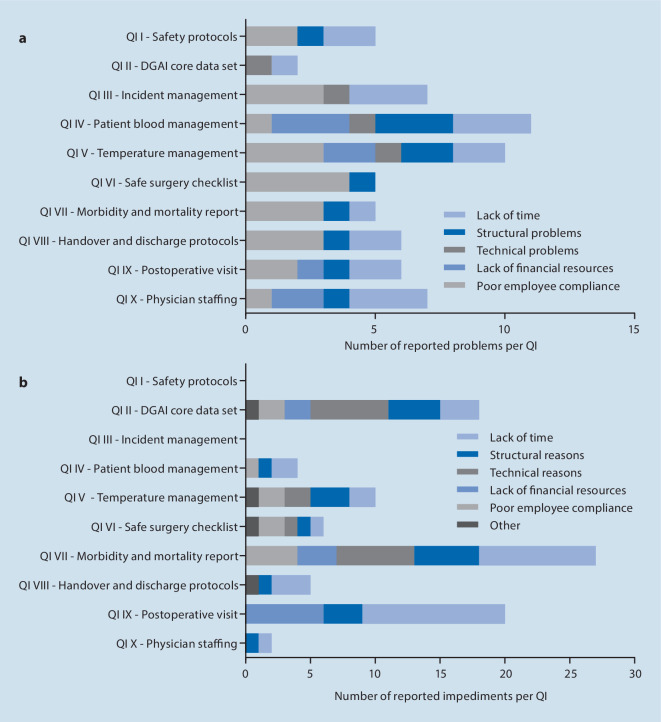
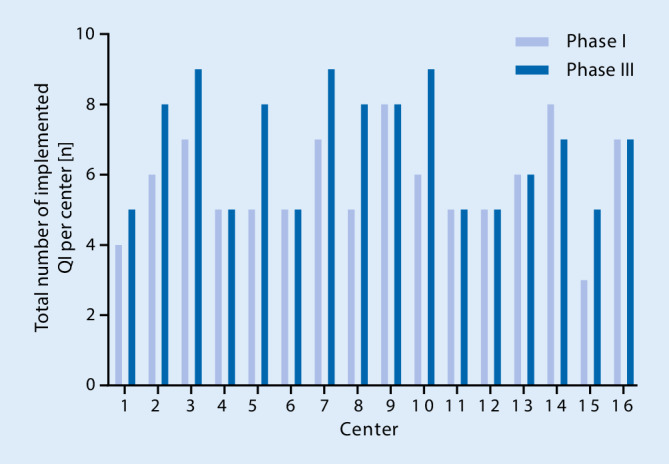
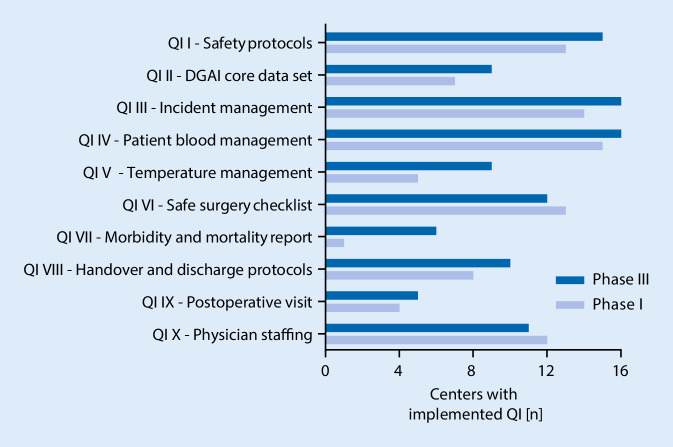
The average number of implemented QI increased from 5.8 to 6.8 (mean of the differences 1.1 ± 1.3; P < 0.01). Most frequently the QI perioperative morbidity and mortality report (5 centers) and the QI temperature management (4 centers) could be implemented. After the implementation phase, the QI incidence management and patient blood management were implemented in all 16 centers. Implementation of other quality indicators failed mainly due to a lack of time and lack of structural resources.
In this study the implementation of QI was proven to be mostly feasible in the participating German hospitals. Although several QI could be implemented with minor effort, more time, financial and structural resources would be required for some QI, such as the QI postoperative visit.
2016 年,德国麻醉学会和重症监护医学学会(DGAI)与德国麻醉师协会(BDA)发布了 10 项质量指标(QI),以比较和提高德国麻醉护理质量。到目前为止,还没有证据表明这些 QI 在医院的实施是可行的。
本研究旨在检验在德国医院实施这 10 项 QI 是可行的假设。
这是一项前瞻性的三阶段全国多中心质量改进研究,于 2017 年 3 月至 2018 年 2 月在德国的 15 家医院和 1 家门诊麻醉中心进行。该试验包括参与麻醉部门负责人对现有结构和流程的初步评估,然后是 QI 的 6 个月实施阶段和最终重新评估阶段。实施过程得到了基于网络的实施辅助工具(www.qi-an.org)和内部质量管理计划的支持。主要终点是每个中心实施前后实施的 QI 数量差异。次要终点是每个中心新实施的 QI 数量、每个 QI 成功实施的总数、实施过程中发现的问题以及阻碍 QI 实施的障碍类型。
每个中心实施的 QI 数量从 5.8 增加到 6.8(平均值差异为 1.1±1.3;P<0.01)。最常实施的 QI 是围手术期发病率和死亡率报告(5 个中心)和体温管理(4 个中心)。实施阶段后,16 个中心都实施了发病率管理和患者血液管理。其他质量指标的实施主要由于缺乏时间和结构性资源而失败。
本研究证明,在参与的德国医院中,QI 的实施大多是可行的。尽管一些 QI 可以通过较小的努力来实施,但对于一些 QI,如术后访问,还需要更多的时间、财务和结构性资源。