Nuventra Pharma Sciences, Durham, North Carolina, USA.
Clin Pharmacol Ther. 2020 Oct;108(4):762-765. doi: 10.1002/cpt.1889. Epub 2020 Jun 7.
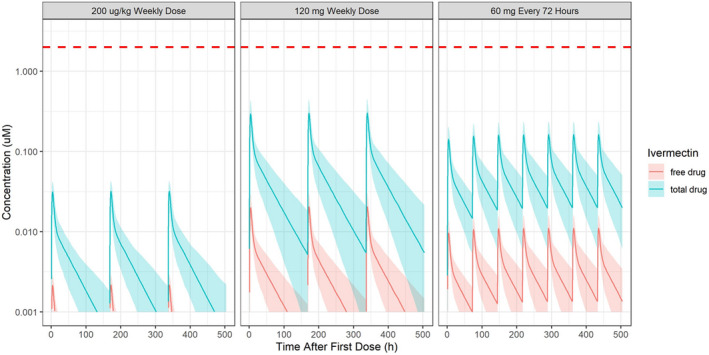
Caly et al. reported that ivermectin inhibited severe acute respiratory syndrome-coronavirus 2 (SARS-CoV-2) in vitro for up to 48 hours using ivermectin at 5 μM. The concentration resulting in 50% inhibition (IC ; 2 µM) was > 35× higher than the maximum plasma concentration (C ) after oral administration of the approved dose of ivermectin when given fasted. Simulations were conducted using an available population pharmacokinetic model to predict total (bound and unbound) and unbound plasma concentration-time profiles after a single and repeat fasted administration of the approved dose of ivermectin (200 μg/kg), 60 mg, and 120 mg. Plasma total C was determined and then multiplied by the lung:plasma ratio reported in cattle to predict the lung C after administration of each single dose. Plasma ivermectin concentrations of total (bound and unbound) and unbound concentrations do not reach the IC , even for a dose level 10× higher than the approved dose. Even with the high lung:plasma ratio, ivermectin is unlikely to reach the IC in the lungs after single oral administration of the approved dose (predicted lung: 0.0873 µM) or at doses 10× higher that the approved dose administered orally (predicted lung: 0.820 µM). In summary, the likelihood of a successful clinical trial using the approved dose of ivermectin is low. Combination therapy should be evaluated in vitro. Repurposing drugs for use in coronavirus disease 2019 (COVID-19) treatment is an ideal strategy but is only feasible when product safety has been established and experiments of repurposed drugs are conducted at clinically relevant concentrations.
Caly 等人报告称,在 5μM 的伊维菌素作用下,体外实验中伊维菌素可抑制严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)长达 48 小时。在禁食状态下给予批准剂量的伊维菌素后,达到 50%抑制浓度(IC ;2μM)所需的浓度(C )比最大血浆浓度高出 35 倍以上。利用现有的群体药代动力学模型进行了模拟,以预测在禁食状态下单次和重复给予批准剂量(200μg/kg)、60mg 和 120mg 伊维菌素后,总(结合和未结合)和未结合的血浆浓度-时间曲线。测定了血浆总 C,然后乘以在牛中报告的肺:血浆比值,以预测每次单剂量给药后的肺 C。总(结合和未结合)和未结合的血浆伊维菌素浓度都未达到 IC ,即使剂量水平比批准剂量高 10 倍也是如此。即使肺:血浆比值高,批准剂量单次口服后,伊维菌素也不太可能达到肺部的 IC (预测肺部:0.0873μM),或者口服剂量比批准剂量高 10 倍(预测肺部:0.820μM)。总之,使用批准剂量的伊维菌素进行成功临床试验的可能性很低。应评估联合疗法。重新利用药物治疗 2019 年冠状病毒病(COVID-19)是一种理想的策略,但只有在产品安全性得到确立且在临床相关浓度下进行重新利用药物的实验时才可行。