Devasenapathy Niveditha, Malhotra Rajesh, Mittal Kanchan, Garg Bhavuk, Kumar Vijay, Zodpey Sanjay, Dogra Hardik, Maddison Ralph, Belavy Daniel L
Indian Institute of Public Health-Delhi, Public Health Foundation of India, New Delhi, India, and Deakin University, Geelong, Victoria, Australia.
All India Institute of Medical Sciences, New Delhi, India.
ACR Open Rheumatol. 2020 Jun;2(6):309-319. doi: 10.1002/acr2.11137. Epub 2020 May 9.
Higher level impairments and activity limitation among those scheduled for total knee arthroplasty (TKA) is known. Sex differences in participation restriction which is the final domain of disablement pathway is not known. No data from developing countries exist on sex differences in disability levels at the time of TKA.
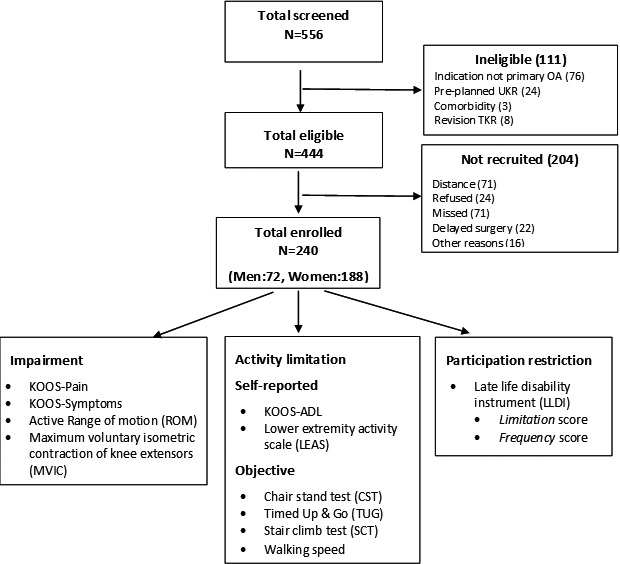
In a cross-sectional analysis of 240 patients (188 women; 72 men) scheduled for TKA, impairment (pain, symptoms, quadricep muscle strength, and knee range of motion [ROM]), activity limitation (self-reported and objective performance-based measurements), and participation restriction were compared. Multivariable regression analyses were used to adjust for key sociodemographic and clinical characteristics. Associations between impairments and participation restriction were analyzed.
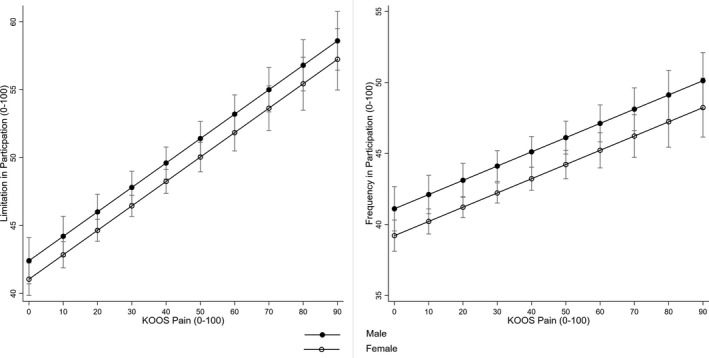
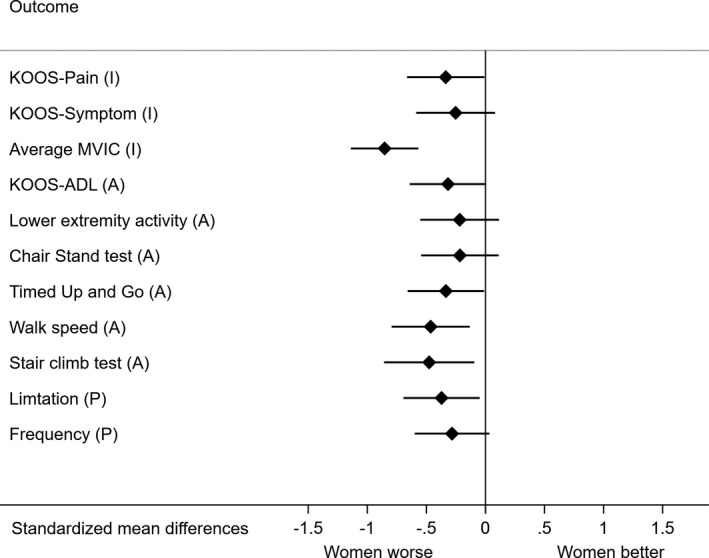
Compared with men, women were more likely to have higher levels of impairment (knee injury and osteoarthritis outcome pain score adjusted mean difference [aMD]: -6.9 [95% confidence interval {CI} -13.7 to -0.18]; flexion ROM of less than 100° adjusted odds ratio: 5.7 [95% CI 1.6-20.3]; and 36% lower muscle strength [95% CI 24%-49%]) and lower objectively measured functional ability (walking speed aMD: -0.12 m/s [95% CI -0.23 to -0.02]; stair climbing time aMD: 9.5 s [95% CI 1.5-17.5]). Participation restriction was higher in women compared with men. Of the impairment measures (pain, ROM, and muscle strength), pain contributed to participation restriction in both sexes.
This study demonstrated higher levels of disability in women than in men at the time of TKA. Effect of pain on participation restriction was higher compared with muscle strength and ROM. Evidence of delay in decision-making to undergo TKA and reasons for delay need to be studied specifically in the context of lower middle-income countries.
已知计划接受全膝关节置换术(TKA)的患者存在更严重的损伤和活动受限情况。然而,关于参与限制这一残疾路径的最后一个领域的性别差异尚不清楚。目前尚无来自发展中国家关于TKA时残疾水平性别差异的数据。
对240例计划接受TKA的患者(188名女性;72名男性)进行横断面分析,比较损伤(疼痛、症状、股四头肌力量和膝关节活动范围[ROM])、活动受限(自我报告和基于客观表现的测量)以及参与限制情况。采用多变量回归分析来调整关键的社会人口统计学和临床特征。分析损伤与参与限制之间的关联。
与男性相比,女性更有可能有更高水平的损伤(膝关节损伤和骨关节炎结局疼痛评分调整后平均差[aMD]:-6.9[95%置信区间{CI}-13.7至-0.18];屈曲ROM小于100°调整后比值比:5.7[95%CI1.6-20.3];肌肉力量低36%[95%CI24%-49%])以及客观测量的功能能力较低(步行速度aMD:-0.12m/s[95%CI-0.23至-0.02];爬楼梯时间aMD:9.5s[95%CI1.5-17.5])。与男性相比,女性的参与限制更高。在损伤测量指标(疼痛、ROM和肌肉力量)中,疼痛对男女双方的参与限制均有影响。
本研究表明,在TKA时女性的残疾水平高于男性。与肌肉力量和ROM相比,疼痛对参与限制的影响更大。在低收入和中等收入国家的背景下,需要专门研究TKA决策延迟的证据及其延迟原因。