Teeäär Tuuli, Serg Martin, Paapstel Kaido, Vähi Mare, Kals Jaak, Cockcroft John R, Zilmer Mihkel, Eha Jaan, Kampus Priit
Department of Cardiology, Institute of Clinical Medicine, University of Tartu, 8 Puusepa Street, Tartu 50406, Estonia.
Heart Clinic, Tartu University Hospital, 8 Puusepa Street, Tartu 50406, Estonia.
Int J Hypertens. 2020 Apr 26;2020:4259187. doi: 10.1155/2020/4259187. eCollection 2020.
Whether the inferior ability of atenolol to reduce central (aortic) compared to peripheral (brachial) blood pressure (BP) is related to its heart rate (HR)-dependent or -independent effects, or their combination, remains unclear. To provide further mechanistic insight into this topic, we studied the acute effects of atenolol versus nebivolol and ivabradine on systolic blood pressure amplification (SBPA; peripheral systolic BP minus central systolic BP) in a model of sick sinus syndrome patients with a permanent dual-chamber cardiac pacemaker in a nonrandomized single-blind single-group clinical trial.
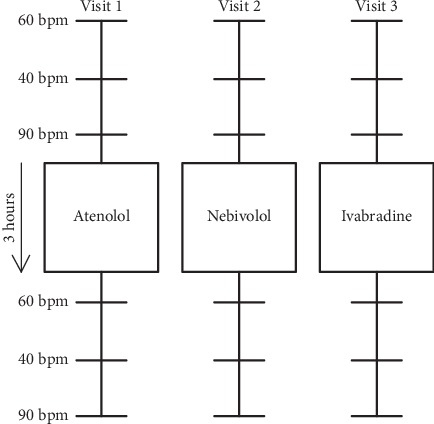
We determined hemodynamic indices noninvasively (Sphygmocor XCEL) before and at least 3 h after administration of oral atenolol 50 or 100 mg, nebivolol 5 mg, or ivabradine 5 or 7.5 mg during atrial pacing at a low (40 bpm), middle (60 bpm), and high (90 bpm) HR level in 25 participants (mean age 65.5 years, 12 men).
At the low HR level, i.e., when the drugs could exert their HR-dependent and HR-independent effects on central BP, only atenolol produced a significant decrease in SBPA (mean change 0.74 ± 1.58 mmHg (95% CI, 0.09-1.40; = 0.028)), indicating inferior central vs peripheral systolic BP change. However, we observed no significant change in SBPA with atenolol at the middle and high HR levels, i.e., when HR-dependent mechanisms had been eliminated by pacing.
The findings of our trial with a mechanistic approach to the topic imply that the inferior ability of atenolol to reduce central vs peripheral BP can be explained by the combination of its heart rate-dependent and -independent effects. This trial is registered with NCT03245996.
与外周(肱动脉)血压相比,阿替洛尔降低中心(主动脉)血压的能力较差,这是否与其心率(HR)依赖性或非依赖性效应,或两者的组合有关,目前尚不清楚。为了进一步深入了解这一主题的机制,我们在一项非随机单盲单组临床试验中,研究了阿替洛尔与奈必洛尔和伊伐布雷定对病态窦房结综合征患者(植入永久性双腔心脏起搏器)收缩压放大(SBPA;外周收缩压减去中心收缩压)的急性影响。
在25名参与者(平均年龄65.5岁,12名男性)中,于低(40次/分钟)、中(60次/分钟)和高(90次/分钟)心率水平进行心房起搏期间,在口服50或100mg阿替洛尔、5mg奈必洛尔或5或7.5mg伊伐布雷定之前和给药后至少3小时,通过无创方式(Sphygmocor XCEL)测定血流动力学指标。
在低心率水平,即当药物可对外周血压发挥其心率依赖性和非依赖性效应时,只有阿替洛尔使SBPA显著降低(平均变化0.74±1.58mmHg(95%CI,0.09 - 1.40;P = 0.028)),表明中心收缩压变化低于外周收缩压变化。然而,在中、高心率水平,即当通过起搏消除心率依赖性机制时,我们观察到阿替洛尔对SBPA无显著变化。
我们对该主题采用机制研究方法的试验结果表明,阿替洛尔降低中心血压与外周血压能力较差可通过其心率依赖性和非依赖性效应的组合来解释。本试验已在ClinicalTrials.gov注册,注册号为NCT03245996。