Department of Radiation oncology and experimental cancer research, Ghent University Hospital, Ghent, Belgium.
Department of Radiation oncology, Iridium Cancer Network, GZ Antwerp, Antwerp, Belgium.
BMC Cancer. 2020 May 12;20(1):406. doi: 10.1186/s12885-020-06911-4.
Pelvic nodal recurrences are being increasingly diagnosed with the introduction of new molecular imaging techniques, like choline and PSMA PET-CT, in the restaging of recurrent prostate cancer (PCa). At this moment, there are no specific treatment recommendations for patients with limited nodal recurrences and different locoregional treatment approaches are currently being used, mostly by means of metastasis-directed therapies (MDT): salvage lymph node dissection (sLND) or stereotactic body radiotherapy (SBRT). Since the majority of patients treated with MDT relapse within 2 years in adjacent lymph node regions, with an estimated median time to progression of 12-18 months, combining MDT with whole pelvic radiotherapy (WPRT) may improve oncological outcomes in these patients. The aim of this prospective multicentre randomized controlled phase II trial is to assess the impact of the addition of WPRT to MDT and short-term androgen deprivation therapy (ADT) on metastasis-free survival (MFS) in the setting of oligorecurrent pelvic nodal recurrence.
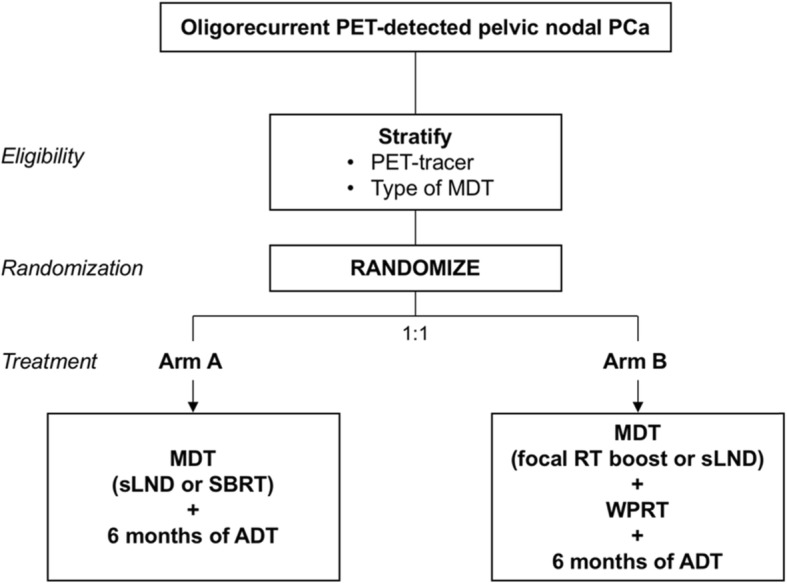
METHODS & DESIGN: Patients diagnosed with PET-detected pelvic nodal oligorecurrence (≤5 nodes) following radical local treatment for PCa, will be randomized in a 1:1 ratio between arm A: MDT and 6 months of ADT, or arm B: WPRT added to MDT and 6 months of ADT. Patients will be stratified by type of PET-tracer (choline, FACBC or PSMA) and by type of MDT (sLND or SBRT). The primary endpoint is MFS and the secondary endpoints include clinical and biochemical progression-free survival (PFS), prostate cancer specific survival, quality of life (QoL), toxicity and time to castration-resistant prostate cancer (CRPC) and to palliative ADT. Estimated study completion: December 31, 2023.
This is the first prospective multicentre randomized phase II trial assessing the potential of combined WPRT and MDT as compared to MDT alone on MFS for patients with nodal oligorecurrent PCa.
ClinicalTrials.gov Identifier: NCT03569241, registered June 14, 2018, ; Identifier on Swiss National Clinical Trials Portal (SNCTP): SNCTP000002947, registered June 14, 2018.
随着新型分子成像技术(如胆碱和 PSMA PET-CT)在复发性前列腺癌(PCa)的再分期中的应用,越来越多地诊断出盆腔淋巴结复发。目前,对于局限性淋巴结复发的患者尚无特定的治疗建议,目前正在使用不同的局部区域治疗方法,主要是通过转移导向治疗(MDT):挽救性淋巴结清扫术(sLND)或立体定向体放射治疗(SBRT)。由于大多数接受 MDT 治疗的患者在 2 年内会在邻近的淋巴结区域复发,估计进展时间中位数为 12-18 个月,因此将 MDT 与全盆腔放疗(WPRT)联合使用可能会改善这些患者的肿瘤学结果。这项前瞻性多中心随机对照 II 期试验的目的是评估在寡复发盆腔淋巴结复发的情况下,将 WPRT 联合 MDT 和短期雄激素剥夺治疗(ADT)添加到 MDT 中对无转移生存(MFS)的影响。
在根治性局部治疗 PCa 后,通过 PET 检测诊断出盆腔淋巴结寡复发(≤5 个淋巴结)的患者将按照 1:1 的比例随机分为 A 组:MDT 加 6 个月 ADT,或 B 组:WPRT 加 MDT 加 6 个月 ADT。患者将按 PET 示踪剂(胆碱、FACBC 或 PSMA)类型和 MDT 类型(sLND 或 SBRT)分层。主要终点是 MFS,次要终点包括临床和生化无进展生存期(PFS)、前列腺癌特异性生存期、生活质量(QoL)、毒性、去势抵抗性前列腺癌(CRPC)时间和姑息性 ADT 时间。预计研究完成日期:2023 年 12 月 31 日。
这是第一项评估与单独 MDT 相比,WPRT 和 MDT 联合治疗在具有淋巴结寡复发 PCa 的患者中对 MFS 的潜在影响的前瞻性多中心 II 期试验。
ClinicalTrials.gov 标识符:NCT03569241,于 2018 年 6 月 14 日注册;瑞士国家临床试验门户网站(SNCTP)上的标识符:SNCTP000002947,于 2018 年 6 月 14 日注册。